You might also like
- Pembahasan TambahanDocument3 pagesPembahasan TambahanNadya Noor Mulya PutriNo ratings yet
- Itinerary Bangkok!!!!!Document5 pagesItinerary Bangkok!!!!!Nadya Noor Mulya PutriNo ratings yet
- CASE REPORT PTHERIGYUM GRADE III-IV OD & II-III OSDocument24 pagesCASE REPORT PTHERIGYUM GRADE III-IV OD & II-III OSNadya Noor Mulya PutriNo ratings yet
- Presentation 3Document1 pagePresentation 3Nadya Noor Mulya PutriNo ratings yet
- Neurology - Spinal Cord PDFDocument1 pageNeurology - Spinal Cord PDFNadya Noor Mulya PutriNo ratings yet
- Jadwal Jaga IpdDocument13 pagesJadwal Jaga IpdNadya Noor Mulya PutriNo ratings yet
- 160 498 1 PB PDFDocument14 pages160 498 1 PB PDFNadya Noor Mulya PutriNo ratings yet
- TetanusDocument23 pagesTetanusNadya Noor Mulya Putri100% (1)
- 5228 10112 1 SMDocument7 pages5228 10112 1 SMNadya Noor Mulya PutriNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hang Tuah Medical Journal: Research ArtikelDocument9 pagesHang Tuah Medical Journal: Research ArtikelMaymay DamayNo ratings yet
- Respiratory System ExplainedDocument48 pagesRespiratory System ExplainedMary Jane LubricoNo ratings yet
- Sensorium.: NiirDocument6 pagesSensorium.: NiirSundar RajanNo ratings yet
- Cellular Respiration AP POGILDocument7 pagesCellular Respiration AP POGILPhil NanceNo ratings yet
- 2nd QUARTER SUMMATIVE TEST FOR PE AND HEALTH 12Document4 pages2nd QUARTER SUMMATIVE TEST FOR PE AND HEALTH 12ANGELYN TI-ADNo ratings yet
- Cardiac Function TestDocument8 pagesCardiac Function Testramanrajesh83100% (2)
- Test 2Document3 pagesTest 2umairgulNo ratings yet
- Multiple Organ Dysfunction Syndrome: HistoryDocument6 pagesMultiple Organ Dysfunction Syndrome: HistoryJasmine BaduaNo ratings yet
- Respiratory System Treatment Modalities Guide (PDFDocument1 pageRespiratory System Treatment Modalities Guide (PDFAdri SinclaireNo ratings yet
- Nebivolol Hydrochlorothiazide Prescribing InformationDocument7 pagesNebivolol Hydrochlorothiazide Prescribing InformationRaihan RakibNo ratings yet
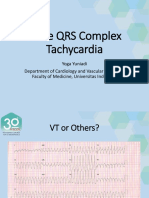
- Yoga Yuniadi - Wide QRS Complex Tachycardia - BaruDocument59 pagesYoga Yuniadi - Wide QRS Complex Tachycardia - BaruZulhelmiNo ratings yet
- CHF DR Arif Case ReportDocument38 pagesCHF DR Arif Case ReportAsakura AyaneNo ratings yet
- Hydrostatic Skeleton PDFDocument4 pagesHydrostatic Skeleton PDFLovie10 KourNo ratings yet
- ACLS Megacode AlgorithmDocument2 pagesACLS Megacode AlgorithmPeter LeeNo ratings yet
- Case StudyDocument7 pagesCase StudyBiway RegalaNo ratings yet
- 1424Document13 pages1424Caiden HenryNo ratings yet
- L - 28-Composition and Function of Blood. ( (L32) )Document28 pagesL - 28-Composition and Function of Blood. ( (L32) )Turky TurkyNo ratings yet
- Biological Psychology Kalat 12th Edition Solutions ManualDocument12 pagesBiological Psychology Kalat 12th Edition Solutions ManualJames Pennington100% (35)
- Assessment Diagnosis Inference Planning Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Inference Planning Intervention Rationale EvaluationMr. whiteNo ratings yet
- EKG - Premature Ventricular Contractions (PVCS)Document8 pagesEKG - Premature Ventricular Contractions (PVCS)SAM dabombdigNo ratings yet
- Major Organ SystemsDocument14 pagesMajor Organ Systemsvinotha kuppusamyNo ratings yet
- Blood CoagulationDocument10 pagesBlood CoagulationgauravkokraNo ratings yet
- (Studies in The History of Modern Science 12) Paul Lawrence Farber (Auth.) - The Emergence of Ornithology As A Scientific Discipline - 1760-1850-Springer Netherlands (1982)Document210 pages(Studies in The History of Modern Science 12) Paul Lawrence Farber (Auth.) - The Emergence of Ornithology As A Scientific Discipline - 1760-1850-Springer Netherlands (1982)janalacerdaNo ratings yet
- Muscle Tissue LabDocument2 pagesMuscle Tissue LabAce MozcareNo ratings yet
- Science6 Q2 Mod3 ExplainHowTheDifferentOrganSystemWorksTogether V4Document24 pagesScience6 Q2 Mod3 ExplainHowTheDifferentOrganSystemWorksTogether V4Jonel BuergoNo ratings yet
- Effects of Sleep Deprivation On The Academic Performance of Senior High School StudentsDocument61 pagesEffects of Sleep Deprivation On The Academic Performance of Senior High School StudentsAngie ZowieNo ratings yet
- Arianna Mabunga Bsn-3BDocument7 pagesArianna Mabunga Bsn-3BArianna Jasmine MabungaNo ratings yet
- HSB - Lesson A1Document31 pagesHSB - Lesson A1Osmany MadrigalNo ratings yet
- Types of ExerciseDocument1 pageTypes of ExerciseTrisha MenesesNo ratings yet
- SAIRUI E-COMMERCE Product CatalogueDocument23 pagesSAIRUI E-COMMERCE Product CatalogueCanaan GamelifeNo ratings yet