You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Dosage Calculation Practice Test 1Document3 pagesDosage Calculation Practice Test 1KamilleAnne KaelaniMaliyaNo ratings yet
- DMFT Index and Dental Caries DetectionDocument56 pagesDMFT Index and Dental Caries DetectionCarolinePiskeNo ratings yet
- L. A. Geddes ME, PHD Auth. Handbook of Blood Pressure MeasurementDocument171 pagesL. A. Geddes ME, PHD Auth. Handbook of Blood Pressure MeasurementYashNo ratings yet
- Assessing Childrens Well-Being A Handbook of Measures ISBN0805831738 PDFDocument325 pagesAssessing Childrens Well-Being A Handbook of Measures ISBN0805831738 PDFFlorentina-Alina CondoiuNo ratings yet
- Basics of Neonatal Ventilation 1Document42 pagesBasics of Neonatal Ventilation 1Abid Ali Rizvi100% (1)
- Orthodontic AnchorageDocument8 pagesOrthodontic Anchoragetderiaty100% (1)
- A Multi-Disciplinary Approach To Class III Therapy Using The Delta Force and ALF Appliances in Conjunction With Terminal Arch ExtractionsDocument4 pagesA Multi-Disciplinary Approach To Class III Therapy Using The Delta Force and ALF Appliances in Conjunction With Terminal Arch ExtractionsOrtho OrganizersNo ratings yet
- Full Report - ELISA LatestDocument8 pagesFull Report - ELISA LatestNik AmirNo ratings yet
- Fuller Et Al-2014-British Journal of DermatologyDocument10 pagesFuller Et Al-2014-British Journal of DermatologyPamelaNo ratings yet
- (Romanian Neurosurgery) Commonly Available CT Characteristics and Prediction of Outcome in Traumatic Brain Injury PatientsDocument11 pages(Romanian Neurosurgery) Commonly Available CT Characteristics and Prediction of Outcome in Traumatic Brain Injury PatientsAinun Nisa Nur CahyatikaNo ratings yet
- Referensi KulitDocument10 pagesReferensi KulitAinun Nisa Nur CahyatikaNo ratings yet
- JurnalDocument6 pagesJurnalAinun Nisa Nur CahyatikaNo ratings yet
- Jurnal Tetanus Case ReportDocument4 pagesJurnal Tetanus Case ReportAinun Nisa Nur CahyatikaNo ratings yet
- JurnalDocument12 pagesJurnalAinun Nisa Nur CahyatikaNo ratings yet
- Otitis Media AafpDocument9 pagesOtitis Media AafpAinun Nisa Nur CahyatikaNo ratings yet
- Agaricus MuscariusDocument25 pagesAgaricus MuscariusFrank NavaNo ratings yet
- Head Injury Draft Full Guideline2 PDFDocument283 pagesHead Injury Draft Full Guideline2 PDFDea Sudiyantika PutriNo ratings yet
- Medical Sales RepresentativeDocument3 pagesMedical Sales Representativeapi-77860217No ratings yet
- Paediatric NeuroanaesthesiaDocument28 pagesPaediatric Neuroanaesthesiakoolstarone100% (1)
- DH SOP LaQshyaDocument81 pagesDH SOP LaQshyakparasher100% (1)
- Apert Syndrome: A Case ReportDocument8 pagesApert Syndrome: A Case ReportIJAR JOURNALNo ratings yet
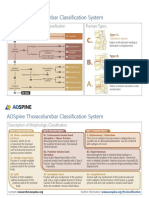
- AOSpine Thoracolumbar Classification System - Pocket CardDocument2 pagesAOSpine Thoracolumbar Classification System - Pocket CardFernanda Ahumada0% (1)
- Cardiopulmonary Resuscitation in Low-Resource SettingsDocument10 pagesCardiopulmonary Resuscitation in Low-Resource SettingsVICTORIA GONZALES ESPADANo ratings yet
- Aging, Muscle Activity, and Balance Control: Physiologic Changes Associated With Balance ImpairmentDocument8 pagesAging, Muscle Activity, and Balance Control: Physiologic Changes Associated With Balance ImpairmentFrancisco Vicent PachecoNo ratings yet
- Does The UNOS Heart Transplant Allocation System Favor Men Over Women?Document9 pagesDoes The UNOS Heart Transplant Allocation System Favor Men Over Women?Thumper KatesNo ratings yet
- Aesculap Basic Sets of Neurosurgical Instruments PDFDocument10 pagesAesculap Basic Sets of Neurosurgical Instruments PDFyudiNo ratings yet
- List of Instruments For 2nd Year BDSDocument17 pagesList of Instruments For 2nd Year BDSMohammad ShoebNo ratings yet
- Myocardial Bridges Over Interventricular Branches of Coronary ArteriesDocument4 pagesMyocardial Bridges Over Interventricular Branches of Coronary Arterieseditorjmst100% (1)
- Resme Rahul GuptaDocument5 pagesResme Rahul Guptarahul guptaNo ratings yet
- Injectable Drugs GuideDocument1 pageInjectable Drugs GuidenasimhsNo ratings yet
- ASHA Module 7Document87 pagesASHA Module 7Prabir Kumar ChatterjeeNo ratings yet
- Daftar Pustaka Koma dan Kesadaran MenurunDocument2 pagesDaftar Pustaka Koma dan Kesadaran MenurunVictoria BerlianiNo ratings yet
- Clinical Practice Guidelines (CPG) : Process ManualDocument46 pagesClinical Practice Guidelines (CPG) : Process ManualMichie RitchNo ratings yet
- Abo IncompatabilityDocument3 pagesAbo Incompatabilityx483xDNo ratings yet
- Postpartum Eclampsia Clinical Study (IJSRDocument3 pagesPostpartum Eclampsia Clinical Study (IJSRSulabh ShresthaNo ratings yet
- Anatomy and Physiology IIDocument13 pagesAnatomy and Physiology IIAuddyjie Hush67% (3)
- LIFE Kite Flying Sponsorship LetterDocument3 pagesLIFE Kite Flying Sponsorship LetterMarjorie CuaNo ratings yet