You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Using SoapDocument1 pageUsing SoapMichael Wilson50% (2)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Banton BiomechanicsDocument9 pagesBanton BiomechanicsIoan AndraNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Reflections On Freud's The UncannyDocument13 pagesReflections On Freud's The UncannyAthina ZiggyNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Vibrational Nos Ws NotesDocument2 pagesVibrational Nos Ws NotesAmi Patel Mehta100% (1)
- How To Use TED TalksDocument4 pagesHow To Use TED TalksMagalíAcevedoNo ratings yet
- How To Use TED TalksDocument4 pagesHow To Use TED TalksMagalíAcevedoNo ratings yet
- Schore - Modern Attachment Theory The Central Role of Affect PDFDocument12 pagesSchore - Modern Attachment Theory The Central Role of Affect PDFveralynn35100% (2)
- 2120Document285 pages2120NYONGKER100% (2)
- Present and Past Simple Tenses With KeyDocument4 pagesPresent and Past Simple Tenses With KeyMagalíAcevedoNo ratings yet
- Clinical History TakingDocument36 pagesClinical History Takingapi-1964133775% (4)
- Fish Vetting Medicines: Formulary of Fish Treatments (2012) by DR Richmond Loh, The Fish Vet.Document14 pagesFish Vetting Medicines: Formulary of Fish Treatments (2012) by DR Richmond Loh, The Fish Vet.thefishvet100% (1)
- Fractured Femur Case StudyDocument9 pagesFractured Femur Case StudyMitzi BelamideNo ratings yet
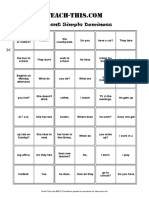
- Present Simple DominoesDocument2 pagesPresent Simple DominoesMagalíAcevedoNo ratings yet
- Session 4 Hand Outs Chapter 2 Counselling Lesson 3-5Document14 pagesSession 4 Hand Outs Chapter 2 Counselling Lesson 3-5Bel Patrice TisuelaNo ratings yet
- MRMDocument39 pagesMRMZafirnur Amrin JasmanNo ratings yet
- Occupational Therapy Evaluation Report and Initial Intervention PlanDocument12 pagesOccupational Therapy Evaluation Report and Initial Intervention Planapi-488383880100% (1)
- Tenses in Medical EnglishDocument1 pageTenses in Medical EnglishMagalíAcevedoNo ratings yet
- Nle Tips MS PDFDocument11 pagesNle Tips MS PDFjthsNo ratings yet
- StereotypesDocument1 pageStereotypesMagalíAcevedoNo ratings yet
- SuperstitionslDocument2 pagesSuperstitionslMagalíAcevedoNo ratings yet
- StereotypesDocument1 pageStereotypesMagalíAcevedoNo ratings yet
- Introducing Yourself A1Document2 pagesIntroducing Yourself A1MagalíAcevedoNo ratings yet
- Holidays: Watch The Video Podcast. Do You Know Any of The Places The People Talk About?Document3 pagesHolidays: Watch The Video Podcast. Do You Know Any of The Places The People Talk About?MagalíAcevedoNo ratings yet
- English Test 1Document2 pagesEnglish Test 1MagalíAcevedoNo ratings yet
- Tests Answer Key Unit 5 Test A : GrammarDocument5 pagesTests Answer Key Unit 5 Test A : GrammarMagalíAcevedoNo ratings yet
- SuperstitionslDocument2 pagesSuperstitionslMagalíAcevedoNo ratings yet
- Big Up For BonobosDocument3 pagesBig Up For BonobosMagalíAcevedoNo ratings yet
- Books and ExperienceDocument1 pageBooks and Experiencehungvu11No ratings yet
- Phrasal Verbs (Unit 11 English File Pre-Intermediate)Document1 pagePhrasal Verbs (Unit 11 English File Pre-Intermediate)MagalíAcevedoNo ratings yet
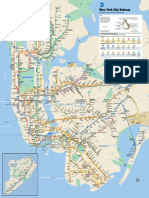
- New York City Subway: THE BronxDocument1 pageNew York City Subway: THE BronxMeraj ShahNo ratings yet
- I) Complete With Do, Don't, Does, Doesn'tDocument2 pagesI) Complete With Do, Don't, Does, Doesn'tMagalíAcevedoNo ratings yet
- Ac TranexamicoDocument8 pagesAc TranexamicoMagalíAcevedoNo ratings yet
- Speaking Cards - ElementaryDocument2 pagesSpeaking Cards - ElementaryMagalíAcevedo100% (1)
- Routines ReadingDocument1 pageRoutines ReadingMagalíAcevedoNo ratings yet
- My Holiday: What Can You Tell About It?Document1 pageMy Holiday: What Can You Tell About It?MagalíAcevedoNo ratings yet
- Sample Us Customs Declaration Form 6059bDocument2 pagesSample Us Customs Declaration Form 6059bmeomeo33No ratings yet
- Present Cont and SimpleDocument3 pagesPresent Cont and SimpleMagalíAcevedoNo ratings yet
- Present Cont and SimpleDocument3 pagesPresent Cont and SimpleMagalíAcevedoNo ratings yet
- Independent Questions SpeakingDocument5 pagesIndependent Questions SpeakingMagalíAcevedoNo ratings yet
- GLOBAL NPV Rate Card December 2016Document7 pagesGLOBAL NPV Rate Card December 2016Gabriel Barriga JaqueNo ratings yet
- Careers: Talk About 2-3 Minutes About CAREERS. Tell About Your Personal Experience. Use The Prompts Below To Help YouDocument1 pageCareers: Talk About 2-3 Minutes About CAREERS. Tell About Your Personal Experience. Use The Prompts Below To Help YouMagalíAcevedoNo ratings yet
- Mind Control Video - ConsciousnessDocument2 pagesMind Control Video - ConsciousnesstanyatewaNo ratings yet
- Guerilla CardioDocument7 pagesGuerilla Cardiomishelll100% (1)
- An Update On The Effect of Clinical Mastitis On The Welfare of Dairy Cows and Potential TherapiesDocument11 pagesAn Update On The Effect of Clinical Mastitis On The Welfare of Dairy Cows and Potential TherapiesLorena PinedaNo ratings yet
- Arum Hastuti Dwi Sofiati Jurnal Persalinan B.inggrisDocument5 pagesArum Hastuti Dwi Sofiati Jurnal Persalinan B.inggrisArum HastutiNo ratings yet
- 2015 Hrinj DrugsDocument303 pages2015 Hrinj Drugsprahul2588100% (1)
- AS R A B A - W T C M C: Hort Eview of Cupuncture and Ronchial Sthma Estern AND Raditional Hinese Edicine OnceptsDocument11 pagesAS R A B A - W T C M C: Hort Eview of Cupuncture and Ronchial Sthma Estern AND Raditional Hinese Edicine Onceptsaprilia ciet cietNo ratings yet
- Mechanical Therapy: by Nikola TeslaDocument2 pagesMechanical Therapy: by Nikola TeslaRommy RahmansyahNo ratings yet
- TDE - Flip-Flop KineticsDocument31 pagesTDE - Flip-Flop KineticsKumar GalipellyNo ratings yet
- Chronopharmacology 120325134521 Phpapp02Document35 pagesChronopharmacology 120325134521 Phpapp02Selva Rathinam0% (1)
- Ellis 1999 REBT Cognitii IrationaleDocument25 pagesEllis 1999 REBT Cognitii IrationaleAlexandra Alexe100% (1)
- Active Cycle of Breathing TechniqueDocument3 pagesActive Cycle of Breathing TechniqueSurya KalaNo ratings yet
- PHAR 7633 Chapter 19 Multi-Compartment Pharmacokinetic ModelsDocument23 pagesPHAR 7633 Chapter 19 Multi-Compartment Pharmacokinetic ModelsBandameedi RamuNo ratings yet
- DK - Falls and Gait DisordersDocument20 pagesDK - Falls and Gait DisordersFahreza KautsarNo ratings yet
- Hand Book Cardiovascular 2018 19-5-18 FinalDocument110 pagesHand Book Cardiovascular 2018 19-5-18 FinalAgim KrasniqiNo ratings yet
- 10 1 1 823 6398 PDFDocument5 pages10 1 1 823 6398 PDFDian Novita AnggraeniNo ratings yet
- Module 9 - Urinary EliminationDocument4 pagesModule 9 - Urinary EliminationPaulette Poseskie CoatesNo ratings yet
- Hyperurecimia and GoutDocument3 pagesHyperurecimia and GoutSunshine_Bacla_4275No ratings yet