You might also like
- West Visayas State University: Nursing ProcessDocument4 pagesWest Visayas State University: Nursing ProcessPhylum Chordata100% (1)
- LESSON 1 Basic Home Care NursingDocument28 pagesLESSON 1 Basic Home Care Nursing1-PASCUAL, Patricia Nicole P.No ratings yet
- CWP Health History Questionnaire Rev 11-17-08Document6 pagesCWP Health History Questionnaire Rev 11-17-08sura srikanthNo ratings yet
- Chapter 4 - Health and Illness ReportDocument30 pagesChapter 4 - Health and Illness ReportRomzy BasañesNo ratings yet
- Physical FitnessDocument2 pagesPhysical FitnessRaj UshamollaNo ratings yet
- Inestabilidad de Hombro Evaluacion y TratamientoDocument13 pagesInestabilidad de Hombro Evaluacion y Tratamientomarcelogascon.oNo ratings yet
- 2 Night Mental Health Program The Farm at San BenitoDocument6 pages2 Night Mental Health Program The Farm at San BenitoArch John DellomaNo ratings yet
- Medical History QuestionnaireDocument3 pagesMedical History QuestionnairefazirapaddamNo ratings yet
- Physician Certification Form 080814Document5 pagesPhysician Certification Form 080814Jeff WilliamsNo ratings yet
- Central Philippine Adventist CollegeDocument5 pagesCentral Philippine Adventist CollegeChede Anne Chonette RoblesNo ratings yet
- Ortho Week 1Document24 pagesOrtho Week 1Jamie John EsplanadaNo ratings yet
- Oswestry Disability Index (ODI)Document3 pagesOswestry Disability Index (ODI)Mohamed ZakiNo ratings yet
- Medical History QuestionnaireDocument3 pagesMedical History QuestionnaireDre EzNo ratings yet
- 7055the BasicsDocument264 pages7055the Basicsdelacruzshaznay444No ratings yet
- Nursing Diagnoses in Psyciatric PDFDocument734 pagesNursing Diagnoses in Psyciatric PDFEgi MunandarNo ratings yet
- Inestabilidad Anterior HombroDocument13 pagesInestabilidad Anterior Hombromarcelogascon.oNo ratings yet
- Salmorin - ACTIVITY 3 - CESocSci4a - Recognizing OpportunitiesDocument2 pagesSalmorin - ACTIVITY 3 - CESocSci4a - Recognizing OpportunitiesBashracel100% (1)
- Attachment Ayrin P. Santos 5-31-2023 9-45-25 AMDocument2 pagesAttachment Ayrin P. Santos 5-31-2023 9-45-25 AMsantosashley.teamjarellNo ratings yet
- CATIMBANG - NAMORO CGA Summary of ReportDocument3 pagesCATIMBANG - NAMORO CGA Summary of ReportJohn Lloyd NamoroNo ratings yet
- My O&g Clerking TemplateDocument8 pagesMy O&g Clerking TemplateFarah FadzilNo ratings yet
- P A-FormatDocument4 pagesP A-FormatKaye Honeylee ManibogNo ratings yet
- Rosebu: Anne Arundel County Maryland Ostomy Association, Ine. P.O.Box 847 Gambrills, MD 21054Document10 pagesRosebu: Anne Arundel County Maryland Ostomy Association, Ine. P.O.Box 847 Gambrills, MD 21054janicewinters7760No ratings yet
- Reason For Home Health Care VisitDocument4 pagesReason For Home Health Care VisitPagodNo ratings yet
- Case Study Diabetic FootDocument38 pagesCase Study Diabetic FootSanti Moore100% (1)
- CX Headache SharmannDocument14 pagesCX Headache SharmannJasmine ShahNo ratings yet
- Lgarlick Client Assessment 12 11 23Document9 pagesLgarlick Client Assessment 12 11 23api-641670151No ratings yet
- Medical Report: Reason RequestedDocument4 pagesMedical Report: Reason RequestedWebmaster0% (1)
- Athlete Registration Medical Concussion 5-13-2021Document7 pagesAthlete Registration Medical Concussion 5-13-2021api-737184619No ratings yet
- Advocate HandbookDocument3 pagesAdvocate Handbookapi-447166621No ratings yet
- Va Offsite DocumentationDocument3 pagesVa Offsite Documentationapi-606438593No ratings yet
- Case Study Repaired)Document30 pagesCase Study Repaired)eelyenoh18100% (1)
- Lincod, Chelly Andrie B. Data Management in Cons. (Cem04) Homework 2 Ceit-02-802E Engr. Ernel FilipinasDocument2 pagesLincod, Chelly Andrie B. Data Management in Cons. (Cem04) Homework 2 Ceit-02-802E Engr. Ernel FilipinasRin KutaruNo ratings yet
- Leadership MGMTDocument3 pagesLeadership MGMTAirglow GNo ratings yet
- PA 1 1 MergedDocument9 pagesPA 1 1 MergedMarc Mhel DalipeNo ratings yet
- Application CoopMED Health Insurance Plan BarbadosDocument2 pagesApplication CoopMED Health Insurance Plan BarbadosKammieNo ratings yet
- NCPChronic PainDocument3 pagesNCPChronic PainArone SebastianNo ratings yet
- Geriatric Assmt ToolDocument9 pagesGeriatric Assmt ToolANITTA SNo ratings yet
- Page 3 6 MHR PRESCREEN QUESTIONNAIREDocument5 pagesPage 3 6 MHR PRESCREEN QUESTIONNAIREMark Joel AguilaNo ratings yet
- 4NC RLE Group 3 - ACTIVITY 2 - CASE SCENARIODocument20 pages4NC RLE Group 3 - ACTIVITY 2 - CASE SCENARIOSofia Franz SabioNo ratings yet
- 386332Document7 pages386332Marcelo BenitezNo ratings yet
- Family Case Guide For InterviewDocument7 pagesFamily Case Guide For Interviewcandy ricel pascuaNo ratings yet
- Medical History Report Medical Prescreen Questionnaire: Philippine National Police Health ServiceDocument3 pagesMedical History Report Medical Prescreen Questionnaire: Philippine National Police Health ServiceJan Vincent A. LadresNo ratings yet
- Gordons Caminade - DoxDocument4 pagesGordons Caminade - DoxZachary CaminadeNo ratings yet
- Fxs FactpublichealthchallengeDocument2 pagesFxs FactpublichealthchallengeandreeaandrioaeNo ratings yet
- 72: Detecting, Assessing, & Responding To Elder MistreatmentDocument16 pages72: Detecting, Assessing, & Responding To Elder Mistreatmentdianaali5No ratings yet
- Senior LivingDocument3 pagesSenior Livingkparsons938512No ratings yet
- Ego Integrity Vs Despair (Comp App)Document10 pagesEgo Integrity Vs Despair (Comp App)Arianne BugnaNo ratings yet
- Terjemahan 3 - 071727Document25 pagesTerjemahan 3 - 071727Merlin NenosonoNo ratings yet
- Health HistoryDocument7 pagesHealth HistoryAnnapurna DangetiNo ratings yet
- History Taking and Risk Assessment and MSE in PsychiatryDocument37 pagesHistory Taking and Risk Assessment and MSE in PsychiatrySanjay PaudelNo ratings yet
- New Case FormDocument5 pagesNew Case FormHenry Joseph Lizardo AlunesNo ratings yet
- Apgenco 2012 Certificate of Fitness 22032012Document2 pagesApgenco 2012 Certificate of Fitness 22032012Veera ChaitanyaNo ratings yet
- Vdocuments - MX Holistic-DiagnosisDocument21 pagesVdocuments - MX Holistic-DiagnosisanitaNo ratings yet
- DM Case StudyDocument21 pagesDM Case StudyBern TolentinoNo ratings yet
- Insight FrailtyDocument8 pagesInsight FrailtyPPDS Rehab Medik UnhasNo ratings yet
- December 2010Document10 pagesDecember 2010janicewinters7760No ratings yet
- For Health: A Health & Wellness GuideDocument24 pagesFor Health: A Health & Wellness GuideDavid ArndtNo ratings yet
- ISS Packet Operation On 70cm-20161113Document1 pageISS Packet Operation On 70cm-20161113tom2susanNo ratings yet
- The Kit Carson TrailDocument4 pagesThe Kit Carson Trailtom2susanNo ratings yet
- Chokes and Shot PatternDocument5 pagesChokes and Shot Patterntom2susanNo ratings yet
- Enron: The Good, The Bad, The LessonsDocument20 pagesEnron: The Good, The Bad, The Lessonstom2susanNo ratings yet
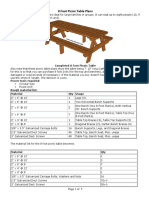
- 8 Foot Picnic Table PlansDocument5 pages8 Foot Picnic Table Planstom2susanNo ratings yet
- Bandanas Carryout MenuDocument3 pagesBandanas Carryout Menutom2susanNo ratings yet
- BabbosDocument2 pagesBabbostom2susanNo ratings yet
- Cloud ChartDocument2 pagesCloud Charttom2susanNo ratings yet
- Panera 2018Document4 pagesPanera 2018tom2susanNo ratings yet
- Thyroid Nodules TI-RADSDocument1 pageThyroid Nodules TI-RADStom2susanNo ratings yet
- Federal Explosives Law and Regulations 2012 Atf-P-5400-7 PDFDocument112 pagesFederal Explosives Law and Regulations 2012 Atf-P-5400-7 PDFtom2susanNo ratings yet
- Therapeutic Shoes For Persons With Diabetes PresentationDocument67 pagesTherapeutic Shoes For Persons With Diabetes Presentationtom2susanNo ratings yet
- Bennett Spring Hatch ChartDocument1 pageBennett Spring Hatch Charttom2susanNo ratings yet
- Blue CardDocument1 pageBlue Cardtom2susanNo ratings yet
- ABI CodingDocument2 pagesABI Codingtom2susanNo ratings yet
- VA Housebound Form VBA-21-2680Document2 pagesVA Housebound Form VBA-21-2680tom2susanNo ratings yet
- Arduino For Ham Radio PresentationDocument50 pagesArduino For Ham Radio Presentationtom2susan100% (2)
- Pyrotechnics - Weingart 1947 PDFDocument247 pagesPyrotechnics - Weingart 1947 PDFtom2susanNo ratings yet
- Cansat2017 5235 CDR v02Document185 pagesCansat2017 5235 CDR v02tom2susanNo ratings yet
- 2015 AMMC (SUMMER) Student HandoutDocument84 pages2015 AMMC (SUMMER) Student Handouttom2susanNo ratings yet
- Animal Science PowerpointDocument104 pagesAnimal Science Powerpointtom2susanNo ratings yet
- SB 656 PassedDocument49 pagesSB 656 Passedtom2susanNo ratings yet
- Personal Fitness MBDocument14 pagesPersonal Fitness MBtom2susanNo ratings yet
- 1recent ExamsDocument42 pages1recent Examsfamilymedicine1234No ratings yet
- Biology - Unit 4 Kingdom ProtistaDocument0 pagesBiology - Unit 4 Kingdom Protistawww.bhawesh.com.npNo ratings yet
- Online Forum - The LobotomistDocument12 pagesOnline Forum - The LobotomistSyakila HanimNo ratings yet
- Daniel Defoe - History of The Plague 1665Document402 pagesDaniel Defoe - History of The Plague 1665differenttraditionsNo ratings yet
- Module 6 - Review AnswersDocument3 pagesModule 6 - Review AnswersKate100% (1)
- Lymphatic System DiseasesDocument1 pageLymphatic System DiseasesRJ San JuanNo ratings yet
- Medical Reimbursement AptranscoDocument13 pagesMedical Reimbursement AptranscopenusilaNo ratings yet
- Early Onset SchizophreniaDocument3 pagesEarly Onset SchizophreniaDoc Prince CaballeroNo ratings yet
- Afriwardi: Bagian Fisiologi Fakultas Kedokteran Universitas Andalas PadangDocument35 pagesAfriwardi: Bagian Fisiologi Fakultas Kedokteran Universitas Andalas PadangAlvin ArifNo ratings yet
- VentilatorDocument90 pagesVentilatorthenaloveNo ratings yet
- Introduction of Acupuncture in Medical PracticeDocument49 pagesIntroduction of Acupuncture in Medical PracticeAnonymous 5IUoLwGSd100% (1)
- Gastroparesis. ACGDocument45 pagesGastroparesis. ACGNaser EsmailiNo ratings yet
- NCM 112 Rle Care of Client With Alteration in Oxygenation: A Case Study On: Chronic Obstructive Pulmonary DiseaseDocument24 pagesNCM 112 Rle Care of Client With Alteration in Oxygenation: A Case Study On: Chronic Obstructive Pulmonary DiseaseMadelyn SerneoNo ratings yet
- Mupirocin OintmentDocument8 pagesMupirocin Ointmentapi-3801331100% (1)
- High - Risk PregnancyDocument110 pagesHigh - Risk PregnancyAndre DityaNo ratings yet
- 1 4931693113845481676 PDFDocument590 pages1 4931693113845481676 PDFRene Cardozo100% (4)
- 1.0 Achalasia & Pyloric StenosisDocument1 page1.0 Achalasia & Pyloric StenosisRaman kangNo ratings yet
- Comprehensive Revision Test - Basics 1Document16 pagesComprehensive Revision Test - Basics 1drpnnreddyNo ratings yet
- Endodontic: EmergenciesDocument53 pagesEndodontic: EmergenciesAhmed S. Abu-Haimed100% (1)
- EB-160 Cupping Therapy Encyclopedia - Tamer Shaban-1 PDFDocument225 pagesEB-160 Cupping Therapy Encyclopedia - Tamer Shaban-1 PDFTanuku Net60% (5)
- Case Report Livia IstratescuDocument26 pagesCase Report Livia IstratescuLivia IstratescuNo ratings yet
- Contraindications To Air TravelDocument15 pagesContraindications To Air TravelsDamnNo ratings yet
- Drug StudyDocument6 pagesDrug StudyBadeth BustamanteNo ratings yet
- Naturopathic Case TakingDocument14 pagesNaturopathic Case Takingsohailnoreen5062No ratings yet
- Wang-Orlow2018 Article KeratosisPilarisAndItsSubtypesDocument25 pagesWang-Orlow2018 Article KeratosisPilarisAndItsSubtypesdaily of sinta fuNo ratings yet
- Denagard Amoxicillin MICs For Respiratory PathogensDocument2 pagesDenagard Amoxicillin MICs For Respiratory Pathogensnick224No ratings yet
- Nejm Pcsk9 StudyDocument10 pagesNejm Pcsk9 Studyherbertgur777No ratings yet
- The$Guide$for$Newly$ Graduated$doctor$ $ $ $ $ Collected$By:$ DR - soran$Mohammed$$Gharib$ M.B.CH.B$ $ $ $$ $ $Document210 pagesThe$Guide$for$Newly$ Graduated$doctor$ $ $ $ $ Collected$By:$ DR - soran$Mohammed$$Gharib$ M.B.CH.B$ $ $ $$ $ $Raghib KurdiNo ratings yet
- Hyperemesis Gravidarum: Is An Extreme, Persistent Nausea and Vomiting During PregnancyDocument1 pageHyperemesis Gravidarum: Is An Extreme, Persistent Nausea and Vomiting During PregnancyDarren RobertoNo ratings yet
- Pediatric Case Presentation 1Document4 pagesPediatric Case Presentation 1soso122100% (1)