You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Discrete Mathematics Sets Relations FunctionsDocument15 pagesDiscrete Mathematics Sets Relations FunctionsMuhd FarisNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Norman Perrin-What Is Redaction CriticismDocument96 pagesNorman Perrin-What Is Redaction Criticismoasis115100% (1)
- Planetary DescriptionsDocument6 pagesPlanetary DescriptionsshellymaryaNo ratings yet
- Black-Scholes Excel Formulas and How To Create A Simple Option Pricing Spreadsheet - MacroptionDocument8 pagesBlack-Scholes Excel Formulas and How To Create A Simple Option Pricing Spreadsheet - MacroptionDickson phiriNo ratings yet
- Pathophysiology of Septic ShockDocument19 pagesPathophysiology of Septic ShockRoberto López MataNo ratings yet
- Build Web Application With Golang enDocument327 pagesBuild Web Application With Golang enAditya SinghNo ratings yet
- HTN Emergencies and UrgenciesDocument14 pagesHTN Emergencies and UrgenciesRoberto López MataNo ratings yet
- Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Synopsis of The 2017 American College of Cardiology:American Heart Association Hypertension GuidelineDocument10 pagesPrevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Synopsis of The 2017 American College of Cardiology:American Heart Association Hypertension GuidelineRoberto López MataNo ratings yet
- Top 10 Myths Regarding The Diagnosis and Treatment of CellulitisDocument8 pagesTop 10 Myths Regarding The Diagnosis and Treatment of CellulitisRoberto López MataNo ratings yet
- Hyperglycemic CrisisDocument9 pagesHyperglycemic CrisisRoberto López MataNo ratings yet
- ADA 2018 Diabetes CareDocument150 pagesADA 2018 Diabetes CareRoberto López Mata100% (1)
- 2017 ACC Expert Consensus Decision Pathway For Optimization of Heart Failure TreatmentDocument30 pages2017 ACC Expert Consensus Decision Pathway For Optimization of Heart Failure TreatmentRoberto López MataNo ratings yet
- Uric Acid Is A Strong Risk Marker For Developing Hypertension From PrehypertensionDocument16 pagesUric Acid Is A Strong Risk Marker For Developing Hypertension From PrehypertensionRoberto López MataNo ratings yet
- Best Clinical Practice: AnaphylaxisDocument6 pagesBest Clinical Practice: AnaphylaxisputriNo ratings yet
- Update On The Management of Venous ThromboembolismDocument8 pagesUpdate On The Management of Venous ThromboembolismRoberto López MataNo ratings yet
- Diagnosis and Treatment of HyperkalemiaDocument9 pagesDiagnosis and Treatment of HyperkalemiaRoberto López MataNo ratings yet
- Effects of Acarbose On Cardiovascular and Diabetes Outcomes in Patients With Coronary Heart Disease and Impaired Glucose Tolerance (ACE) - A Randomised, Double-Blind, Placebo-Controlled TrialDocument10 pagesEffects of Acarbose On Cardiovascular and Diabetes Outcomes in Patients With Coronary Heart Disease and Impaired Glucose Tolerance (ACE) - A Randomised, Double-Blind, Placebo-Controlled TrialRoberto López MataNo ratings yet
- Necrotizing Soft-Tissue InfectionsDocument13 pagesNecrotizing Soft-Tissue InfectionsRoberto López MataNo ratings yet
- Fluid Therapy Options and Rational SelectionDocument13 pagesFluid Therapy Options and Rational SelectionRoberto López MataNo ratings yet
- The Role of Nitroglycerin and Other Nitrogen Oxides in Cardiovascular TherapeuticsDocument18 pagesThe Role of Nitroglycerin and Other Nitrogen Oxides in Cardiovascular TherapeuticsRoberto López MataNo ratings yet
- Hepatitis B Vaccination, Screening, and Linkage To Care - Best Practice Advice From The American College of Physicians and The Centers For Disease Control and PreventionDocument12 pagesHepatitis B Vaccination, Screening, and Linkage To Care - Best Practice Advice From The American College of Physicians and The Centers For Disease Control and PreventionRoberto López MataNo ratings yet
- The Use of Cephalosporins in Penicillin-Allergic Patients - A Literature ReviewDocument9 pagesThe Use of Cephalosporins in Penicillin-Allergic Patients - A Literature ReviewRoberto López MataNo ratings yet
- The Dark Sides of Fuid Administration in The Critically Ill PatientDocument3 pagesThe Dark Sides of Fuid Administration in The Critically Ill PatientRoberto López MataNo ratings yet
- Diuretic Treatment in Heart FailureDocument12 pagesDiuretic Treatment in Heart FailureRoberto López Mata100% (1)
- Sudden Cardiac Arrest During Participation in Competitive SportsDocument11 pagesSudden Cardiac Arrest During Participation in Competitive SportsRoberto López MataNo ratings yet
- Rivaroxaban Vs Warfarin Sodium in The Ultra-Early Period After Atrial Fibrillation-Related Mild Ischemic StrokeDocument10 pagesRivaroxaban Vs Warfarin Sodium in The Ultra-Early Period After Atrial Fibrillation-Related Mild Ischemic StrokeRoberto López MataNo ratings yet
- 2015 ESC Guidelines For The Diagnosis and Management of Pericardial DiseasesDocument44 pages2015 ESC Guidelines For The Diagnosis and Management of Pericardial DiseasesRoberto López MataNo ratings yet
- Atrial Fibrillation and HypertensionDocument17 pagesAtrial Fibrillation and HypertensionRoberto López MataNo ratings yet
- A Test in Context - D-DimerDocument10 pagesA Test in Context - D-DimerRoberto López MataNo ratings yet
- Synopsis of The 2017 U.S. Department of Veterans Affairs: Management of Type 2 Diabetes MellitusDocument10 pagesSynopsis of The 2017 U.S. Department of Veterans Affairs: Management of Type 2 Diabetes MellitusRoberto López MataNo ratings yet
- Effects on the Incidence of Cardiovascular Events of the Addition of Pioglitazone Versus Sulfonylureas in Patients With Type 2 Diabetes Inadequately Controlled With Metformin (TOSCA.it)- A Randomised, Multicentre TrialDocument11 pagesEffects on the Incidence of Cardiovascular Events of the Addition of Pioglitazone Versus Sulfonylureas in Patients With Type 2 Diabetes Inadequately Controlled With Metformin (TOSCA.it)- A Randomised, Multicentre TrialRoberto López MataNo ratings yet
- Dual Antithrombotic Therapy With Dabigatran After PCI in Atrial FibrillationDocument12 pagesDual Antithrombotic Therapy With Dabigatran After PCI in Atrial FibrillationRoberto López MataNo ratings yet
- Acute Monocular Vision LossDocument9 pagesAcute Monocular Vision LossRoberto López MataNo ratings yet
- Evaluation and Management of Lower-Extremity UlcersDocument9 pagesEvaluation and Management of Lower-Extremity UlcersRoberto López MataNo ratings yet
- Verification ofDocument14 pagesVerification ofsamuel-kor-kee-hao-1919No ratings yet
- Andrew Haywood CV 2010Document6 pagesAndrew Haywood CV 2010Dobber0No ratings yet
- E-WasteDocument18 pagesE-WasteNitinKotwarNo ratings yet
- Sample PREP-31 Standard Sample Preparation Package For Rock and Drill SamplesDocument1 pageSample PREP-31 Standard Sample Preparation Package For Rock and Drill SampleshNo ratings yet
- It'S Not A Lie If You Believe It: LyingDocument2 pagesIt'S Not A Lie If You Believe It: LyingNoel ll SorianoNo ratings yet
- 14-) NonLinear Analysis of A Cantilever Beam PDFDocument7 pages14-) NonLinear Analysis of A Cantilever Beam PDFscs1720No ratings yet
- Advanced Signal Multi-ScannerDocument8 pagesAdvanced Signal Multi-ScannerneerajupmanyuNo ratings yet
- NationalMootCourtCompetition Moot ProblemDocument5 pagesNationalMootCourtCompetition Moot ProblemKarsin ManochaNo ratings yet
- Reformer Tube Inspection: Leo - ScanDocument5 pagesReformer Tube Inspection: Leo - ScanAnonymous 5odj1IcNo ratings yet
- Effects of Temperature and Moisture On SMCDocument20 pagesEffects of Temperature and Moisture On SMCsenencostasNo ratings yet
- Botbee IntegrationDocument16 pagesBotbee IntegrationAnuj VikalNo ratings yet
- Microelectronic CircuitsDocument22 pagesMicroelectronic CircuitsarunnellurNo ratings yet
- Qualifications Recruitment Promotions Scheme - University AcademicsDocument10 pagesQualifications Recruitment Promotions Scheme - University Academicsuteachers_slNo ratings yet
- Alpha-Qwerty Cipher: An Extended Vigenere CipherDocument12 pagesAlpha-Qwerty Cipher: An Extended Vigenere CipherAnonymous IlrQK9HuNo ratings yet
- MCVM: Monte Carlo Modeling of Photon Migration in Voxelized MediaDocument12 pagesMCVM: Monte Carlo Modeling of Photon Migration in Voxelized MediaĐô Lê PhiNo ratings yet
- Binary RelationDocument9 pagesBinary RelationDavidNo ratings yet
- Jillin ExplosionDocument10 pagesJillin ExplosionArjun ManojNo ratings yet
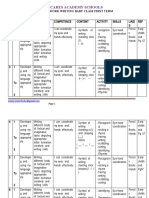
- Scheme of Work Writing Baby First TermDocument12 pagesScheme of Work Writing Baby First TermEmmy Senior Lucky100% (1)
- Mexico For Sale. Rafael GuerreroDocument12 pagesMexico For Sale. Rafael GuerreroGabriela Durán ValisNo ratings yet
- DfgtyhDocument4 pagesDfgtyhAditya MakkarNo ratings yet
- 4D Asp: Wall Tiling 4D - PG 1Document3 pages4D Asp: Wall Tiling 4D - PG 1Vlaho AlamatNo ratings yet
- Academics: Qualification Institute Board/University Year %/CGPADocument1 pageAcademics: Qualification Institute Board/University Year %/CGPARajesh KandhwayNo ratings yet
- Role of ICT & Challenges in Disaster ManagementDocument13 pagesRole of ICT & Challenges in Disaster ManagementMohammad Ali100% (3)
- Name: Period: Date:: Math Lab: Explore Transformations of Trig Functions Explore Vertical DisplacementDocument7 pagesName: Period: Date:: Math Lab: Explore Transformations of Trig Functions Explore Vertical DisplacementShaaminiNo ratings yet
- Nexlinx Corporate Profile-2019Document22 pagesNexlinx Corporate Profile-2019sid202pkNo ratings yet