You might also like
- Service Animal LawsDocument14 pagesService Animal LawsherushingNo ratings yet
- Estate of Tomas Beauford v. Mesa County, Colorado, Et. Al.Document45 pagesEstate of Tomas Beauford v. Mesa County, Colorado, Et. Al.Michael_Lee_RobertsNo ratings yet
- Physical Framework AntiqueDocument279 pagesPhysical Framework AntiqueSerafin Yanga100% (1)
- Reducing Poverty in Myanmar - DR U MyintDocument23 pagesReducing Poverty in Myanmar - DR U Myintpaylaypin100% (2)
- Personal Financial Planning Case Study for Ahmad in 2013-2046Document50 pagesPersonal Financial Planning Case Study for Ahmad in 2013-2046Jahid Hasan100% (5)
- Faqs On The Parole Process For Cubans Haitians Nicaraguans and Venezuelans.2023.01.18Document11 pagesFaqs On The Parole Process For Cubans Haitians Nicaraguans and Venezuelans.2023.01.18Antonio PerezNo ratings yet
- From Neglect To RespectDocument8 pagesFrom Neglect To RespectMental Health Reform100% (1)
- R.A. 9275 - Philippine Clean Water Act of 2004Document19 pagesR.A. 9275 - Philippine Clean Water Act of 2004Ma Jhunelle A. BaduaNo ratings yet
- Community Health WorkersDocument42 pagesCommunity Health WorkersSathya PalanisamyNo ratings yet
- Health Referral System Manual - Central VisayasDocument103 pagesHealth Referral System Manual - Central VisayasAlfred Russel Wallace50% (10)
- Make Decisions: NPA Discussion - NHS White Paper. 28 Jul 2010Document4 pagesMake Decisions: NPA Discussion - NHS White Paper. 28 Jul 2010Idrees MohammedNo ratings yet
- Clinical Data Quality ProcedureDocument17 pagesClinical Data Quality Procedurejhonron100% (1)
- A Junior Doctor's NHS: Guide To TheDocument15 pagesA Junior Doctor's NHS: Guide To ThemickbazNo ratings yet
- Kaiser Volunteer ApplicationDocument6 pagesKaiser Volunteer ApplicationVanessa HoNo ratings yet
- Community-Oriented Primary Care (COPC) in District Health Services of Gauteng, South AfricaDocument4 pagesCommunity-Oriented Primary Care (COPC) in District Health Services of Gauteng, South AfricaAileyIrvetteNo ratings yet
- Community Oriented Primary Care COPC in District Health Services of Gauteng South AfricaDocument4 pagesCommunity Oriented Primary Care COPC in District Health Services of Gauteng South AfricaKim G. SarongNo ratings yet
- Berwick Top 10 TipsDocument3 pagesBerwick Top 10 TipsmnovemberNo ratings yet
- Community Health WorkersDocument42 pagesCommunity Health WorkersGeethaNambiar100% (1)
- Shaping Personal Health Budgets A View From The TopDocument24 pagesShaping Personal Health Budgets A View From The Toptony_jameson-allenNo ratings yet
- Personal Health Budgets Report July 2014Document4 pagesPersonal Health Budgets Report July 2014NHSOpenhouseNo ratings yet
- Health Care Reform Term PaperDocument10 pagesHealth Care Reform Term Paperafmzxppzpvoluf100% (1)
- Discussion Paper 1: Enshrining The Ability To Work in The New NHS, Steve BoormanDocument9 pagesDiscussion Paper 1: Enshrining The Ability To Work in The New NHS, Steve BoormanFitForWorkUKNo ratings yet
- Intelligent Kindness: Reforming The Culture of HealthcareDocument7 pagesIntelligent Kindness: Reforming The Culture of Healthcarefarnaz_2647334No ratings yet
- Innovate, Co-Operate To Improve Health Services For CanadiansLet's Be More Than A Nation of Pilot Projects'by Kimberlyn McGrailDocument2 pagesInnovate, Co-Operate To Improve Health Services For CanadiansLet's Be More Than A Nation of Pilot Projects'by Kimberlyn McGrailEvidenceNetwork.caNo ratings yet
- Collaborative Healthcare - IC FinalDocument11 pagesCollaborative Healthcare - IC FinalInclusionNorthNo ratings yet
- Nsach Community AssessmentDocument8 pagesNsach Community Assessmentapi-311766385No ratings yet
- 2008 Annual ReportDocument36 pages2008 Annual ReportVir NaffaNo ratings yet
- 5yfv Web PDFDocument41 pages5yfv Web PDFjonNo ratings yet
- Module 4 2Document4 pagesModule 4 2api-642701476No ratings yet
- Hsci 6250Document4 pagesHsci 6250api-642711495No ratings yet
- Innovation Health and Wealth Report 2012dh - 134597Document36 pagesInnovation Health and Wealth Report 2012dh - 134597Alejandro CardonaNo ratings yet
- CBRT PHC Report May09Document52 pagesCBRT PHC Report May09Bryan tsepang NareNo ratings yet
- HA Convention Opening SpeechDocument8 pagesHA Convention Opening SpeechwakakaNo ratings yet
- Improving Rural Primary Care with Nurse PractitionersDocument2 pagesImproving Rural Primary Care with Nurse Practitionersraffickbowen2731No ratings yet
- National Health Service Organisational and Management Issues February 20101Document5 pagesNational Health Service Organisational and Management Issues February 20101Brian FisherNo ratings yet
- PPPs Key to Healthcare for All in IndiaDocument31 pagesPPPs Key to Healthcare for All in IndiasubbarajuNo ratings yet
- Community Health Workers in Health Care For The Homeless: A Guide For AdministratorsDocument14 pagesCommunity Health Workers in Health Care For The Homeless: A Guide For AdministratorsretnoNo ratings yet
- Pharmacy Action Plan 2016 To 2020 PDFDocument48 pagesPharmacy Action Plan 2016 To 2020 PDFssenpharma9934No ratings yet
- NHS Future Forum: Summary Report On Proposed Changes To The NHSDocument31 pagesNHS Future Forum: Summary Report On Proposed Changes To The NHSIan DuntNo ratings yet
- Bab 1 Isian AwalDocument19 pagesBab 1 Isian AwalBakti SetiawanNo ratings yet
- The Administration of Health Services in The Twenty-First CenturyDocument16 pagesThe Administration of Health Services in The Twenty-First CenturyPamela Neyra VeraNo ratings yet
- HEALTH MATTERSDocument2 pagesHEALTH MATTERSHarveyNo ratings yet
- HIS VidDocument8 pagesHIS VidJacqueline HarleNo ratings yet
- MHO Vision & MissionDocument10 pagesMHO Vision & MissionJoEd VillAlonNo ratings yet
- CNA's Primary Health Care ApproachDocument5 pagesCNA's Primary Health Care ApproachÀi ZìjǐNo ratings yet
- Community Health 2 Cat 2Document4 pagesCommunity Health 2 Cat 2samuel mbuguaNo ratings yet
- Planning Human Resources in Health Care: Towards An Economic Approach An International Comparative ReviewDocument34 pagesPlanning Human Resources in Health Care: Towards An Economic Approach An International Comparative ReviewIonelia PașaNo ratings yet
- Cancer Support Initiative Improves AccessDocument3 pagesCancer Support Initiative Improves AccesssigitNo ratings yet
- How Governments Can Improve Health System StewardshipDocument24 pagesHow Governments Can Improve Health System StewardshipnilandariNo ratings yet
- Research (Community Health Center)Document19 pagesResearch (Community Health Center)Luego, Brent Jarryd P.No ratings yet
- CHWs Role in Chronic Disease PreventionDocument13 pagesCHWs Role in Chronic Disease PreventionGift EseNo ratings yet
- Issue Brief 5 CHWsDocument2 pagesIssue Brief 5 CHWsNay Lin HtikeNo ratings yet
- The Health Inequalities Assessment Toolkit: Supporting Integration of Equity Into Applied Health ResearchDocument6 pagesThe Health Inequalities Assessment Toolkit: Supporting Integration of Equity Into Applied Health ResearchAna Porroche-EscuderoNo ratings yet
- National Public Health Institute A Framework For DevelopmentDocument37 pagesNational Public Health Institute A Framework For DevelopmentIslam SaeedNo ratings yet
- MEDSEM JOSTF-P Article: A New Paradigm For SOF Counterinsurgency Medical ProgramsDocument7 pagesMEDSEM JOSTF-P Article: A New Paradigm For SOF Counterinsurgency Medical ProgramsMitchell RosserNo ratings yet
- Review of The Alberta Health Services Organization and Structure, and Next StepsDocument16 pagesReview of The Alberta Health Services Organization and Structure, and Next StepsCTV CalgaryNo ratings yet
- Primary Health Care WHO OverviewDocument16 pagesPrimary Health Care WHO OverviewlilaningNo ratings yet
- Community Based Mental HealthcareDocument4 pagesCommunity Based Mental HealthcarerhiachiNo ratings yet
- NCM 104 Week 3Document15 pagesNCM 104 Week 3Nathan Lloyd SangcapNo ratings yet
- Literature Review of The Cambodian Health Care SystemDocument9 pagesLiterature Review of The Cambodian Health Care SystemafmzsawcpkjfzjNo ratings yet
- Public Health Care ManagementDocument33 pagesPublic Health Care Managementalexandercecilia67No ratings yet
- Healthcast The Customisation of Diagnosis Care and Cure-Pwc-2010 PDFDocument58 pagesHealthcast The Customisation of Diagnosis Care and Cure-Pwc-2010 PDFEhli HibreNo ratings yet
- Research Proposal Social Health and Development: Population-Based Managed Care (PBMC) Is A Management Technique DesignedDocument10 pagesResearch Proposal Social Health and Development: Population-Based Managed Care (PBMC) Is A Management Technique DesignedJaved HassanNo ratings yet
- Hss 1Document4 pagesHss 1InterActionNo ratings yet
- Imelda Mcdermott, Lynsey Warwick-Giles, Oz Gore, Valerie Moran, Donna Bramwell, Anna Coleman, and Kath ChecklandDocument11 pagesImelda Mcdermott, Lynsey Warwick-Giles, Oz Gore, Valerie Moran, Donna Bramwell, Anna Coleman, and Kath ChecklandhppnukNo ratings yet
- Issue 13: Cchoht UpdateDocument3 pagesIssue 13: Cchoht UpdateBlakeNo ratings yet
- Efficacy, Effectiveness And Efficiency In The Management Of Health SystemsFrom EverandEfficacy, Effectiveness And Efficiency In The Management Of Health SystemsNo ratings yet
- Accountable Care Organizations: Your Guide to Strategy, Design, and ImplementationFrom EverandAccountable Care Organizations: Your Guide to Strategy, Design, and ImplementationNo ratings yet
- Joint Media StatementDocument1 pageJoint Media StatementTheChronicleHeraldNo ratings yet
- 2016 Statement of Compensation Combined-FINAL-Aug-10-2016Document16 pages2016 Statement of Compensation Combined-FINAL-Aug-10-2016TheChronicleHeraldNo ratings yet
- TicksDocument1 pageTicksTheChronicleHeraldNo ratings yet
- CRA-CH Graphs - Likelihood of Voting - May 11, 2017Document1 pageCRA-CH Graphs - Likelihood of Voting - May 11, 2017TheChronicleHeraldNo ratings yet
- The Government of Canada and The Government of Nova Scotia Reach Agreement Under New Federal Infrastructure Funding ProgramsDocument18 pagesThe Government of Canada and The Government of Nova Scotia Reach Agreement Under New Federal Infrastructure Funding ProgramsTheChronicleHeraldNo ratings yet
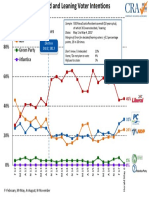
- Final CH Graphs - Leaning and Voter Intentions - May 6, 2017Document1 pageFinal CH Graphs - Leaning and Voter Intentions - May 6, 2017TheChronicleHeraldNo ratings yet
- FINAL CH Graphs - Leader Ratings - May 6 2017Document1 pageFINAL CH Graphs - Leader Ratings - May 6 2017TheChronicleHeraldNo ratings yet
- FINAL CH Graphs - Most Prefer As Premier - May 6 2017Document1 pageFINAL CH Graphs - Most Prefer As Premier - May 6 2017TheChronicleHeraldNo ratings yet
- Infrastructure Projects ListDocument11 pagesInfrastructure Projects ListTheChronicleHeraldNo ratings yet
- Information To Obtain A Warrant To Take Bodily Substances For Forensic DNA AnalysisDocument25 pagesInformation To Obtain A Warrant To Take Bodily Substances For Forensic DNA AnalysisTheChronicleHeraldNo ratings yet
- Yarmouth Ferry ContractDocument18 pagesYarmouth Ferry ContractTheChronicleHeraldNo ratings yet
- South ElevationDocument1 pageSouth ElevationTheChronicleHeraldNo ratings yet
- 10 Day Workout Plan 260cf416 73ce 41ff b8f5 6b38f89aebc9Document6 pages10 Day Workout Plan 260cf416 73ce 41ff b8f5 6b38f89aebc9alexlucu21No ratings yet
- Optima Restore Rate Card PDFDocument2 pagesOptima Restore Rate Card PDFSrinivas GuvvaNo ratings yet
- GMR Airports Signs Concession Agreement For North Goaâ ™s Greenfield International Airport at Mopa (Company Update)Document4 pagesGMR Airports Signs Concession Agreement For North Goaâ ™s Greenfield International Airport at Mopa (Company Update)Shyam SunderNo ratings yet
- Rt5201 Lineside Security PDFDocument8 pagesRt5201 Lineside Security PDFCezary P.No ratings yet
- FakeDocument11 pagesFakearthithaNo ratings yet
- Semi Final Exam For Tax 1Document6 pagesSemi Final Exam For Tax 1Gregorio ReyNo ratings yet
- Japans Population CrisisDocument9 pagesJapans Population Crisisapi-302646839No ratings yet
- Healthcare Reform Timeline For Self-Funded PlansDocument1 pageHealthcare Reform Timeline For Self-Funded PlansPayerFusionNo ratings yet
- Healthcare System at State LevelDocument18 pagesHealthcare System at State LevelAnjali SainiNo ratings yet
- Admin of Meds Prof GuidanceDocument8 pagesAdmin of Meds Prof GuidanceStacyNo ratings yet
- 4-26 Motion To Dismiss SC District CourtDocument2 pages4-26 Motion To Dismiss SC District CourtBasseemNo ratings yet
- International Financial InstitutionsDocument2 pagesInternational Financial Institutionsumerahmad01No ratings yet
- Session 6 Meaning and Nature of RiskDocument20 pagesSession 6 Meaning and Nature of RiskPranit ShahNo ratings yet
- SOP Template v2.1Document3 pagesSOP Template v2.1superagent007No ratings yet
- Community College Initiative (CCI) ProgramDocument2 pagesCommunity College Initiative (CCI) ProgramWilson Marques de Andrade FilhoNo ratings yet
- Central Govt Schemes List AllDocument131 pagesCentral Govt Schemes List AllA INFOTECH mediaNo ratings yet
- Impact of The Covid-19 On PoliticsDocument7 pagesImpact of The Covid-19 On PoliticsJack knightNo ratings yet
- ABILIFY® (Aripiprazole) Savings Card ProgramDocument2 pagesABILIFY® (Aripiprazole) Savings Card ProgramGisele PhaloNo ratings yet
- Candace Steel LawsuitDocument20 pagesCandace Steel LawsuitMichelleNo ratings yet
- Municipal Corporations ActDocument254 pagesMunicipal Corporations ActKrislin SeepersadNo ratings yet
- Special Immigrant Visa Biodata Form 55Document2 pagesSpecial Immigrant Visa Biodata Form 55NoelCabauatanNo ratings yet