You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Inpatient Rehab LTLD Referral GuidelinesDocument8 pagesInpatient Rehab LTLD Referral GuidelinesAdi Kurnia SandiNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Second Week Social Welfare Policies and ProgramsDocument14 pagesSecond Week Social Welfare Policies and ProgramsLea Jane Laurete CalledoNo ratings yet
- Clinical Sports Medicine (4th Edition) - Brukner, KhanDocument1,342 pagesClinical Sports Medicine (4th Edition) - Brukner, KhanJacob Co91% (33)
- Marissa Nurs3021 Midterm EvaluationDocument16 pagesMarissa Nurs3021 Midterm Evaluationapi-372418362No ratings yet
- Worksheet Present Simple and Daily Routines1Document4 pagesWorksheet Present Simple and Daily Routines1TasiaFerreiraNo ratings yet
- CSP Core Standards 2005 0Document68 pagesCSP Core Standards 2005 0Irina MafteiNo ratings yet
- Part I - Listening: 1. Listen and Write Numbers Next To The Parts of The HouseDocument4 pagesPart I - Listening: 1. Listen and Write Numbers Next To The Parts of The HouseTasiaFerreiraNo ratings yet
- Unifying Neuro-Fasciagenic Model ofDocument18 pagesUnifying Neuro-Fasciagenic Model ofTasiaFerreiraNo ratings yet
- Unifying Neuro-Fasciagenic Model ofDocument18 pagesUnifying Neuro-Fasciagenic Model ofTasiaFerreiraNo ratings yet
- English For Physiotherapists 2Document117 pagesEnglish For Physiotherapists 2Artur PacekNo ratings yet
- Clinical Observation ReflectionDocument5 pagesClinical Observation Reflectionapi-270593384No ratings yet
- Recovery Model Paper-RaginsDocument20 pagesRecovery Model Paper-RaginsChris Broomfield100% (1)
- Chapter 1 - Modern Hospital ArchitectureDocument39 pagesChapter 1 - Modern Hospital Architecturemarye agegnNo ratings yet
- Causes and Treatment of Mental Disorder at Talay Rehabilitation CenterDocument22 pagesCauses and Treatment of Mental Disorder at Talay Rehabilitation Centerhershey100% (1)
- ANATOMIA PALPATÓRIA DO MEMBRO SUPERIORDocument9 pagesANATOMIA PALPATÓRIA DO MEMBRO SUPERIORnídia_santos_3No ratings yet
- Adult Learning and Mainstream Education DiscourseDocument24 pagesAdult Learning and Mainstream Education DiscourseTasiaFerreiraNo ratings yet
- Teste 6º Present ContDocument10 pagesTeste 6º Present ContTasiaFerreiraNo ratings yet
- Set 1 Task A.1Document3 pagesSet 1 Task A.1Tânia Patrícia TeixeiraNo ratings yet
- The Role of The SternumDocument14 pagesThe Role of The SternumTasiaFerreiraNo ratings yet
- Set 0. 1Document5 pagesSet 0. 1Tânia Patrícia TeixeiraNo ratings yet
- The Effects of Thoracic Manipulation en Posteroanterior Spinal Stiffness PDFDocument9 pagesThe Effects of Thoracic Manipulation en Posteroanterior Spinal Stiffness PDFTasiaFerreiraNo ratings yet
- Set 0Document9 pagesSet 0TasiaFerreiraNo ratings yet
- Set 1 Task A. 2Document2 pagesSet 1 Task A. 2TasiaFerreiraNo ratings yet
- Set 0 2Document5 pagesSet 0 2Tânia Patrícia TeixeiraNo ratings yet
- Test 3 HouseDocument4 pagesTest 3 HouseTasiaFerreiraNo ratings yet
- Test 3 HouseDocument4 pagesTest 3 HouseTasiaFerreiraNo ratings yet
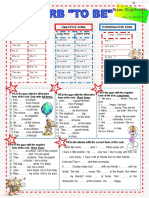
- 1 - Ficha de Trabalho - To BeDocument1 page1 - Ficha de Trabalho - To BeMariliaReganhaNo ratings yet
- Unit: Prepositions of PlaceDocument6 pagesUnit: Prepositions of PlaceAdalia López PNo ratings yet
- 1 - Ficha de Trabalho - To BeDocument1 page1 - Ficha de Trabalho - To BeMariliaReganhaNo ratings yet
- What's in the Office - 6th Grade English TestDocument6 pagesWhat's in the Office - 6th Grade English TestTasiaFerreiraNo ratings yet
- MainDocument15 pagesMainJesusNavarrete97No ratings yet
- Electro Therapy Equipment-Firing EVODocument1 pageElectro Therapy Equipment-Firing EVOImam TaufikNo ratings yet
- The FIM System Clinical GuideDocument180 pagesThe FIM System Clinical GuideNoora BurshidNo ratings yet
- Facial PalsyDocument7 pagesFacial PalsyPedro FonsecaNo ratings yet
- Court upholds finality of judgment in personal injury caseDocument9 pagesCourt upholds finality of judgment in personal injury casebergs daotNo ratings yet
- PIN2763 Thoracic Spine ExercisesDocument3 pagesPIN2763 Thoracic Spine ExercisesShamsuddin Hasnani100% (1)
- Worksheet CCJM Post OpDocument3 pagesWorksheet CCJM Post Opapi-631170779No ratings yet
- Compensation Benefits Types Compared Across Canadian ProvincesDocument6 pagesCompensation Benefits Types Compared Across Canadian ProvincesJansen GunardiNo ratings yet
- Department of Labor: 0205wccaDocument21 pagesDepartment of Labor: 0205wccaUSA_DepartmentOfLaborNo ratings yet
- Press Release FS Announced FINALDocument4 pagesPress Release FS Announced FINALDrDylanMNo ratings yet
- 1 s2.0 S0020748920302546 MainDocument12 pages1 s2.0 S0020748920302546 MainAnnisa Nur RamadhaniNo ratings yet
- Regulatory Guidelines For ExoskeletonDocument27 pagesRegulatory Guidelines For Exoskeletondipys41No ratings yet
- Te'aja Praylow: Seeking Entry-Level Occupational Therapy PositionDocument2 pagesTe'aja Praylow: Seeking Entry-Level Occupational Therapy Positionapi-540029997No ratings yet
- Demonstration and Evlauation of Enset Corm Ensete Venrticosum Based Oxen Fattening in Kachabira and Lemu Districts Southern EthiopiaDocument5 pagesDemonstration and Evlauation of Enset Corm Ensete Venrticosum Based Oxen Fattening in Kachabira and Lemu Districts Southern EthiopiaHerald Scholarly Open AccessNo ratings yet
- Introduction To Hospital AdministrationDocument17 pagesIntroduction To Hospital AdministrationPrasidha PrabhuNo ratings yet
- Injury Prevention For RunnersDocument12 pagesInjury Prevention For RunnersMulaNo ratings yet
- DN 0423 1606Document9 pagesDN 0423 1606JayannaNo ratings yet
- Maitry Chheda: Ug 2020 - PresentDocument2 pagesMaitry Chheda: Ug 2020 - PresentMaitryChhedaNo ratings yet
- Evidence To Practice Review Best Practices in Patellar Tendinopathy ManagementDocument8 pagesEvidence To Practice Review Best Practices in Patellar Tendinopathy ManagementLeandroNo ratings yet
- Models of Rehabilitation Component IA Role Name Affiliation: Swe/Swfd/Mr/M23 by Dr. P. Saleel KumarDocument13 pagesModels of Rehabilitation Component IA Role Name Affiliation: Swe/Swfd/Mr/M23 by Dr. P. Saleel KumarRainbowsNo ratings yet