You might also like
- When No Is No - Voluntary ChildnessDocument12 pagesWhen No Is No - Voluntary ChildnessHelena AlexandraNo ratings yet
- Drugclasses Pharmacologypart 1 PDFDocument25 pagesDrugclasses Pharmacologypart 1 PDFSutanya100% (2)
- In Defense of The Liberal PeaceDocument6 pagesIn Defense of The Liberal PeaceQuinn ZimmermanNo ratings yet
- Differential Diagnosis of The Adnexal Mass 2020Document38 pagesDifferential Diagnosis of The Adnexal Mass 2020Sonia MVNo ratings yet
- Drug Guideline For Iron Polymaltose InjectionDocument7 pagesDrug Guideline For Iron Polymaltose Injectionmirza_baig_46No ratings yet
- Beta-Lactam Compounds Mechanisms of Action and ResistanceDocument2 pagesBeta-Lactam Compounds Mechanisms of Action and ResistanceJayde TabanaoNo ratings yet
- Administering Vaccines To AdultsDocument1 pageAdministering Vaccines To AdultsPaul Anthony LoricaNo ratings yet
- Pharmacological Management of Pulmonary EmbolismDocument49 pagesPharmacological Management of Pulmonary EmbolismDaniela Rojas CorreaNo ratings yet
- Fetal MonitoringDocument28 pagesFetal MonitoringLina MartinezNo ratings yet
- Cardiovascular DiseasesDocument8 pagesCardiovascular DiseasesRebecca MarshallNo ratings yet
- Summary of Medicine in MalaysiaDocument50 pagesSummary of Medicine in MalaysiagohyichengNo ratings yet
- Drug Classificati On Indications Action Route/Dos e Side Effects Patient Teaching Nursing ImplicationsDocument7 pagesDrug Classificati On Indications Action Route/Dos e Side Effects Patient Teaching Nursing ImplicationsJenny NguyenNo ratings yet
- Update On The Management of Venous ThromboembolismDocument8 pagesUpdate On The Management of Venous ThromboembolismRoberto López MataNo ratings yet
- Burn Stabilization ProtocolDocument2 pagesBurn Stabilization ProtocolAli AftabNo ratings yet
- Reducing Maternal Mortality: Theories, Models, and PracticeDocument17 pagesReducing Maternal Mortality: Theories, Models, and PracticeRavi Pamnani100% (2)
- Protein Calorie MalnutritionDocument97 pagesProtein Calorie Malnutritionnshaikh56No ratings yet
- Common Prefixes and SuffixesDocument5 pagesCommon Prefixes and Suffixestriddle1969100% (1)
- Primary Care Antibiotic Guideline FINAL May 2015Document10 pagesPrimary Care Antibiotic Guideline FINAL May 2015Atta Muhammad MemonNo ratings yet
- PG PREPARATION - Mnemonics in PharmacologyDocument12 pagesPG PREPARATION - Mnemonics in PharmacologyRaveen KumarNo ratings yet
- Drugs in Blood DisordersDocument1 pageDrugs in Blood DisordersSantosh patelNo ratings yet
- Pulmonary Tuberculos IS: PGI Aquino Ruel Aldrin PGI Andaman Greg JinichiDocument79 pagesPulmonary Tuberculos IS: PGI Aquino Ruel Aldrin PGI Andaman Greg JinichiIggs AndamanNo ratings yet
- Approach To The Patient With An Adnexal Mass - UpToDateDocument31 pagesApproach To The Patient With An Adnexal Mass - UpToDateRamackNo ratings yet
- Massive Transfusion ProtocolDocument2 pagesMassive Transfusion ProtocolmukriNo ratings yet
- Placement and Management of Thoracostomy Tubes - UpToDateDocument24 pagesPlacement and Management of Thoracostomy Tubes - UpToDateAndres Felipe Cuspoca OrduzNo ratings yet
- Classification of The DrugsDocument50 pagesClassification of The DrugsGlena SalamNo ratings yet
- If HP Cancer Guide br007 MriDocument13 pagesIf HP Cancer Guide br007 Mrirusgal8992100% (1)
- Cancer and EnvironmentDocument47 pagesCancer and Environmentandra1982No ratings yet
- PancreatitisDocument2 pagesPancreatitisMary GiuntiniNo ratings yet
- Emergency Drugs Used in O.S. Common Drug Interactions in O.S. Practice Oral SurgeryDocument52 pagesEmergency Drugs Used in O.S. Common Drug Interactions in O.S. Practice Oral SurgeryFourthMolar.comNo ratings yet
- Student Objectives - ACOGDocument164 pagesStudent Objectives - ACOGmango91286100% (1)
- MUT17 Booklet 2Document18 pagesMUT17 Booklet 2baang43farhanNo ratings yet
- Managemant Copd CPG MsiaDocument67 pagesManagemant Copd CPG MsiaNur Anis ZarimeNo ratings yet
- Pharm C Exam 10 Drug ListDocument2 pagesPharm C Exam 10 Drug ListVokdadaNo ratings yet
- Drug Toxicity and PoisoningDocument12 pagesDrug Toxicity and PoisoningPAULA MARIE MERCADO LLIDONo ratings yet
- VOD - SOS in HSCTDocument25 pagesVOD - SOS in HSCTKim-Thinh Nguyen ThiNo ratings yet
- Cisplatin/ 5-Fluorouracil For Squamous Cell Carcinoma Head and Neck (HNSCC) - Day Unit ProtocolDocument6 pagesCisplatin/ 5-Fluorouracil For Squamous Cell Carcinoma Head and Neck (HNSCC) - Day Unit Protocoldwi harisNo ratings yet
- National Guideline for Clinical Management of Dengue SyndromeDocument96 pagesNational Guideline for Clinical Management of Dengue SyndromeTapash GopeNo ratings yet
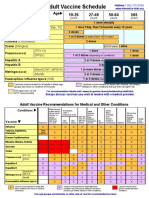
- Adult Vaccine Schedule Eng PDFDocument2 pagesAdult Vaccine Schedule Eng PDFAbdur RehmanNo ratings yet
- Glycogen Storage DiseasesDocument4 pagesGlycogen Storage DiseasesDennis ValdezNo ratings yet
- Ectopic Pregnancy PDFDocument38 pagesEctopic Pregnancy PDFByron Ruiz Lapuerta100% (1)
- BJH Heparin GuidelinesDocument16 pagesBJH Heparin Guidelinesd40sithui100% (1)
- Psychiatry PhyseoDocument60 pagesPsychiatry PhyseoGautam ManoharNo ratings yet
- What Is AchalasiaDocument6 pagesWhat Is AchalasiaDonnaliza Delos ReyesNo ratings yet
- 1 Gastrointestinal EmergenciesDocument142 pages1 Gastrointestinal EmergenciesRashida UmarNo ratings yet
- GEN GallBladderInstrumentsADocument10 pagesGEN GallBladderInstrumentsANeo Rodriguez AlvaradoNo ratings yet
- Heart FailureDocument28 pagesHeart FailureNabeel ShahzadNo ratings yet
- Hematuria in ChildrenDocument26 pagesHematuria in ChildrenNovenZefanya100% (1)
- Emergency Medicine in MBBSDocument85 pagesEmergency Medicine in MBBSPATHMAPRIYA GANESANNo ratings yet
- Pharm Expansion 17 NDFDocument1 pagePharm Expansion 17 NDFNokz M. Raki-inNo ratings yet
- Laproscopic SurgeryDocument80 pagesLaproscopic SurgeryAqeel AhmadNo ratings yet
- (Pha) Le 5Document19 pages(Pha) Le 5Gabby TanNo ratings yet
- Prospectus Nus Diploma Course in Tissue BankingDocument6 pagesProspectus Nus Diploma Course in Tissue BankingAnimat_Me100% (1)
- Birth Defects - PPSXDocument47 pagesBirth Defects - PPSXCharith R Ramesh100% (1)
- Adults With Suspected Epiglottitis - Supraglottitis Guidelines For The Management ofDocument2 pagesAdults With Suspected Epiglottitis - Supraglottitis Guidelines For The Management ofAlexandros MegasNo ratings yet
- Pedia DrugsDocument1 pagePedia DrugseyakoyNo ratings yet
- Maternal Collapse During PregnancyDocument57 pagesMaternal Collapse During PregnancytapayanaNo ratings yet
- Combined Hormone Pill, Patch, Ring Progestin Only Mini Pill, Depo-Provera, IUDDocument1 pageCombined Hormone Pill, Patch, Ring Progestin Only Mini Pill, Depo-Provera, IUDnkuligowskiNo ratings yet
- Non Steroidal Anti Inflammatory DrugDocument21 pagesNon Steroidal Anti Inflammatory DrugRanganath NagarajNo ratings yet
- Risk PDFDocument50 pagesRisk PDFErick Antonio Castillo GurdianNo ratings yet
- Non-Opioid DrugsDocument40 pagesNon-Opioid DrugsifaNo ratings yet
- Cutaneous Changes in Venous and Lymphatic InsufficiencyDocument4 pagesCutaneous Changes in Venous and Lymphatic InsufficiencyAlmas PrawotoNo ratings yet
- Hidronefrosis PDFDocument54 pagesHidronefrosis PDFAlmas PrawotoNo ratings yet
- Condiloma AkuminataDocument3 pagesCondiloma AkuminataAlmas PrawotoNo ratings yet
- Condiloma AkuminataDocument3 pagesCondiloma AkuminataAlmas PrawotoNo ratings yet
- Journal Ischemic StrokeDocument9 pagesJournal Ischemic StrokeAlmas PrawotoNo ratings yet
- Why Is Long-Term Therapy Required To Cure Tuberculosis?: Research in TranslationDocument8 pagesWhy Is Long-Term Therapy Required To Cure Tuberculosis?: Research in TranslationMonica Herdiati Rukmana NaibahoNo ratings yet
- Diabetes in TeensDocument5 pagesDiabetes in TeensAlmas PrawotoNo ratings yet
- Journal Reading IKK ANHDocument15 pagesJournal Reading IKK ANHAlmas PrawotoNo ratings yet
- Identifying Risk For Diabetes in Adolescence (Irda) : A Pilot Study in General PracticeDocument12 pagesIdentifying Risk For Diabetes in Adolescence (Irda) : A Pilot Study in General PracticeAlmas PrawotoNo ratings yet
- Hawaii Travel PlanDocument103 pagesHawaii Travel PlanAlmas PrawotoNo ratings yet
- Bab 1Document2 pagesBab 1Almas PrawotoNo ratings yet
- Official Reprint From Uptodate ©2017 UptodateDocument9 pagesOfficial Reprint From Uptodate ©2017 UptodateAlmas Prawoto100% (1)
- Hawaii Hotel NumberDocument1 pageHawaii Hotel NumberAlmas PrawotoNo ratings yet
- Perioperative Planning & Pain ManagementDocument18 pagesPerioperative Planning & Pain ManagementAlmas PrawotoNo ratings yet
- Oxford Perioperative Pain Management 2013Document141 pagesOxford Perioperative Pain Management 2013Almas PrawotoNo ratings yet
- Guideline PresbycusisDocument4 pagesGuideline PresbycusisAlmas PrawotoNo ratings yet
- OsteomyelitisDocument5 pagesOsteomyelitisAlmas PrawotoNo ratings yet
- Interpretasi RontgenDocument12 pagesInterpretasi RontgenAlmas PrawotoNo ratings yet
- Meniscus Injury: Almas PrawotoDocument9 pagesMeniscus Injury: Almas PrawotoAlmas PrawotoNo ratings yet
- Anterior Cruciate Ligament InjuriesDocument16 pagesAnterior Cruciate Ligament InjuriesAlmas PrawotoNo ratings yet
- Official Reprint From Uptodate ©2017 UptodateDocument9 pagesOfficial Reprint From Uptodate ©2017 UptodateAlmas Prawoto100% (1)
- Damage ControlDocument8 pagesDamage ControlAlmas PrawotoNo ratings yet
- Fracture ManagementDocument4 pagesFracture ManagementAlmas PrawotoNo ratings yet
- Fracture ManagementDocument4 pagesFracture ManagementAlmas PrawotoNo ratings yet
- Post TraumaDocument5 pagesPost TraumaAlmas PrawotoNo ratings yet
- WSH guidelines diagnose manage occupational diseasesDocument106 pagesWSH guidelines diagnose manage occupational diseasesmediaaprina100% (1)
- CH 19 Nursing Care of Patients With Immune System DisordersDocument2 pagesCH 19 Nursing Care of Patients With Immune System DisordersZachary T Hall0% (1)
- Lab Technician or Clerical or BankingDocument2 pagesLab Technician or Clerical or Bankingapi-76931734No ratings yet
- Article - Quick REMAP - Steps in The Quick REMAP4-point Rapid Relief Protocol 1 PDFDocument32 pagesArticle - Quick REMAP - Steps in The Quick REMAP4-point Rapid Relief Protocol 1 PDFAnonymous g8zT2sPtjW100% (1)
- Hydrocephalus UpdatesDocument65 pagesHydrocephalus Updatescddinchimm100% (1)
- Newcastle Satisfaction With Nursing Scales AnDocument6 pagesNewcastle Satisfaction With Nursing Scales AnlemootpNo ratings yet
- CC.14.01 Pre and Post Operative CareDocument3 pagesCC.14.01 Pre and Post Operative CareKrupaNo ratings yet
- A HOFFER Review Niacin The Real StoryDocument2 pagesA HOFFER Review Niacin The Real StoryAna Lu100% (1)
- LeprosyDocument9 pagesLeprosyJohn Ribu Parampil100% (1)
- 10 Nursing Note SampleDocument1 page10 Nursing Note Sampletesttest testNo ratings yet
- Narrative Report On School Nursing - EditedDocument16 pagesNarrative Report On School Nursing - EditedAbby_Cacho_9151100% (2)
- Acceptance of Dying A Discourse Analysis of Palliative Care LiteratureDocument8 pagesAcceptance of Dying A Discourse Analysis of Palliative Care LiteratureMauricio MartinezNo ratings yet
- Intersect ENT Investor Presentation - $XENTDocument28 pagesIntersect ENT Investor Presentation - $XENTmedtechyNo ratings yet
- LT033 PDFDocument38 pagesLT033 PDFAlexandr ChuvakovNo ratings yet
- Bi PAPDocument30 pagesBi PAPraerlnNo ratings yet
- ParkinsonDocument54 pagesParkinsonAngel YapNo ratings yet
- Tugas 2 BHS Ing Rani OctalyaDocument3 pagesTugas 2 BHS Ing Rani OctalyaRozaq Permana YudhaNo ratings yet
- TNM Staging Colorectal CADocument2 pagesTNM Staging Colorectal CAbubbrubb20063998No ratings yet
- ComplianceDocument13 pagesCompliancextremist2001No ratings yet
- Competency Based EducationDocument33 pagesCompetency Based EducationAncy Varkey100% (1)
- Early Enteral NutritionDocument55 pagesEarly Enteral NutritionAdya ArradikhaNo ratings yet
- Case Presentation - Closed Fracture Radius Ulna PediatricDocument30 pagesCase Presentation - Closed Fracture Radius Ulna PediatriciamboredtiredNo ratings yet
- Anatomy and Types of ScoliosisDocument18 pagesAnatomy and Types of ScoliosisVanessa Yvonne GurtizaNo ratings yet
- International Patient Safety Goals IPSGDocument20 pagesInternational Patient Safety Goals IPSGShafique HussainNo ratings yet
- Current Trends in PharmacovigilanceDocument5 pagesCurrent Trends in PharmacovigilanceSutirtho MukherjiNo ratings yet
- Nursing Assessment For PainDocument9 pagesNursing Assessment For PainNDJNo ratings yet
- Nursing KardexDocument2 pagesNursing Kardexjerimiah_manzon100% (3)
- MED 2 Electrical Safety Test of Medical Equipment After RepairDocument17 pagesMED 2 Electrical Safety Test of Medical Equipment After RepairAfiz86No ratings yet
- Nurs402 Teachingprojectsummary NeuburgDocument20 pagesNurs402 Teachingprojectsummary Neuburgapi-452041818No ratings yet
- Rehabilitation in The Dynamic Stabilization of Lumbar SpineDocument41 pagesRehabilitation in The Dynamic Stabilization of Lumbar SpineYip Song ChongNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- Chakras and Yoga: Finding Inner Harmony Through Practice, Awaken the Energy Centers for Optimal Physical and Spiritual Health.From EverandChakras and Yoga: Finding Inner Harmony Through Practice, Awaken the Energy Centers for Optimal Physical and Spiritual Health.Rating: 4 out of 5 stars4/5 (2)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (4)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (31)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Daniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisFrom EverandDaniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisRating: 3.5 out of 5 stars3.5/5 (130)