You might also like
- TEACHING PLAN HypertensionDocument2 pagesTEACHING PLAN Hypertensionpheochromocytoma59% (41)
- Lessonplan FinDocument14 pagesLessonplan Finx483xDNo ratings yet
- Rain PDFDocument2 pagesRain PDFRadhika Sethu100% (1)
- Network Management System by Man I SubramanianDocument4 pagesNetwork Management System by Man I SubramanianRadhika Sethu0% (1)
- Extra Oral ExaminationDocument19 pagesExtra Oral ExaminationmarwanNo ratings yet
- Lateral Neck SwellingDocument62 pagesLateral Neck Swellingசுபத்ரா சந்திரசேகர்No ratings yet
- An Approach To The Neck Masses: BY: Hardi H. QaderDocument49 pagesAn Approach To The Neck Masses: BY: Hardi H. QaderEmad AlryashiNo ratings yet
- Approach To Patients With LymphadenopathyDocument5 pagesApproach To Patients With LymphadenopathyAngela Mitchelle NyanganNo ratings yet
- Neck MassesDocument24 pagesNeck MassesIstiklal SurgeryNo ratings yet
- Surgical Diseases of The SpleenDocument28 pagesSurgical Diseases of The SpleenRassoul Abu-NuwarNo ratings yet
- Lymph Nodes in The Neck: AnswerDocument7 pagesLymph Nodes in The Neck: AnswerLady Dianne Recabe Severino0% (1)
- SpleenDocument42 pagesSpleenRashed LabNo ratings yet
- Lymphadenopathy: Go ToDocument7 pagesLymphadenopathy: Go ToendahNo ratings yet
- The Third LectureDocument14 pagesThe Third LectureMustafa AliNo ratings yet
- Cyst Neck Tumor (DR Bob Andinata)Document33 pagesCyst Neck Tumor (DR Bob Andinata)Intan Eklesiana NapitupuluNo ratings yet
- BLS - The Detailed Online Five GuideDocument23 pagesBLS - The Detailed Online Five GuidepeterNo ratings yet
- Immune SystemDocument32 pagesImmune SystemZero OrezNo ratings yet
- Adenomegalias 08Document10 pagesAdenomegalias 08Brenda CaraveoNo ratings yet
- 11 - Part1.Neck MassesDocument51 pages11 - Part1.Neck MassesRashed ShatnawiNo ratings yet
- RT 304 Prelim NotesDocument32 pagesRT 304 Prelim NotesNikko L. PescuesoNo ratings yet
- Case VirchowsDocument14 pagesCase VirchowsShanti IntansariNo ratings yet
- Important Features Are: History of Neck SwellingsDocument4 pagesImportant Features Are: History of Neck SwellingsMuqtadir “The Ruler” Kuchiki100% (1)
- Differential Diagnosis of A Neck Mass - UpToDateDocument16 pagesDifferential Diagnosis of A Neck Mass - UpToDatezzellowknifeNo ratings yet
- Common Health Problems in PreschoolersDocument22 pagesCommon Health Problems in PreschoolersClaire Alvarez OngchuaNo ratings yet
- An Approach To Diagnosis: Neck LumpDocument36 pagesAn Approach To Diagnosis: Neck LumpTracy WheelerNo ratings yet
- Immunity 1Document6 pagesImmunity 1Tori RolandNo ratings yet
- LymphomaDocument37 pagesLymphomaMohammed T. Abdul Razak100% (2)
- Lymphatic Drainage of Head and NeckDocument51 pagesLymphatic Drainage of Head and NeckDR NASIMNo ratings yet
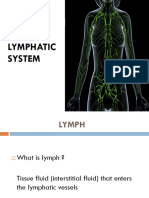
- Lymphatic SystemDocument45 pagesLymphatic SystemNabil Abd El-tawabNo ratings yet
- Kelainan KongenitalDocument20 pagesKelainan KongenitalMelita GanNo ratings yet
- Case Write UpDocument9 pagesCase Write UpAsraf LatifNo ratings yet
- D.D of Mid-Line Neck SwellingsDocument21 pagesD.D of Mid-Line Neck Swellingsmhmdalbdyny764No ratings yet
- Cystic HygromaDocument2 pagesCystic HygromaAmal AlahmariNo ratings yet
- Examination of Lymphatic SystemDocument21 pagesExamination of Lymphatic SystemPankaj KumarNo ratings yet
- Cervical Lymph NodeDocument4 pagesCervical Lymph NodeHermawan HmnNo ratings yet
- Digestive Domain GuideDocument31 pagesDigestive Domain Guidemina000005No ratings yet
- Non-Hodgkin Lymphoma Rhabdomyosarcoma Retinoblastoma: by Derrota, Keith Angelo CDocument39 pagesNon-Hodgkin Lymphoma Rhabdomyosarcoma Retinoblastoma: by Derrota, Keith Angelo CKeith Angelo Canete DerrotaNo ratings yet
- Propedevtika Engleski EtcDocument19 pagesPropedevtika Engleski Etcgrit27No ratings yet
- Examination of Lymph NodesDocument16 pagesExamination of Lymph NodesRose DeymNo ratings yet
- Inguinal LAPDocument12 pagesInguinal LAPDarawan MirzaNo ratings yet
- Pleurisy and Bronchogenic CarcinomaDocument11 pagesPleurisy and Bronchogenic CarcinomaNoemi GarciaNo ratings yet
- Lymphatic - System - HDN 3Document42 pagesLymphatic - System - HDN 3Rashini FernandoNo ratings yet
- SpleenDocument33 pagesSpleenAin AmanyNo ratings yet
- The Lymphatic SystemDocument7 pagesThe Lymphatic SystemPreeti ChouhanNo ratings yet
- BC LesionsDocument7 pagesBC LesionsMuhammad AdelNo ratings yet
- Physical Examination of The Lymphatic System: Russell C Hendershot DO, MS, FAAFPDocument50 pagesPhysical Examination of The Lymphatic System: Russell C Hendershot DO, MS, FAAFPNajwa100% (1)
- Laporan Kasus VI Bahasa InggrisDocument10 pagesLaporan Kasus VI Bahasa InggrisWahyu SholekhuddinNo ratings yet
- Leukemia Cells & ColorectalDocument40 pagesLeukemia Cells & ColorectalYum CNo ratings yet
- Hydrocephalus: Prepared By: Sita PariyarDocument38 pagesHydrocephalus: Prepared By: Sita PariyarSarita PariyarNo ratings yet
- Common Neck SwellingsDocument54 pagesCommon Neck SwellingsMpanso Ahmad AlhijjNo ratings yet
- Kelainan Kepala Dan LeherDocument17 pagesKelainan Kepala Dan LeherSoraya HumairaNo ratings yet
- Neck Mass ProtocolDocument8 pagesNeck Mass ProtocolCharlene FernándezNo ratings yet
- Neck LumpDocument18 pagesNeck LumpJosh BurkeNo ratings yet
- Examination of Lymph NodesDocument16 pagesExamination of Lymph Nodeslokesh_045No ratings yet
- Lymph NodesDocument6 pagesLymph NodesIsak ShatikaNo ratings yet
- Conditions of The Lymph SystemDocument37 pagesConditions of The Lymph Systemkurage_07No ratings yet
- 4 2Document3 pages4 2Stefia AisyahNo ratings yet
- Neck Lumps, (Cervical Masses) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandNeck Lumps, (Cervical Masses) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Superior Vena Cava Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandSuperior Vena Cava Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Carpal Tunnel Syndrome, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandCarpal Tunnel Syndrome, A Simple Guide To The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Pleural Effusion, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandPleural Effusion, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- What About Sweets?: Nutrition SeriesDocument2 pagesWhat About Sweets?: Nutrition SeriesRadhika SethuNo ratings yet
- Feeding RabbitDocument22 pagesFeeding RabbitRadhika SethuNo ratings yet
- Skill 47 (1) ..Tracheostomy Tube Change PDFDocument2 pagesSkill 47 (1) ..Tracheostomy Tube Change PDFRadhika SethuNo ratings yet
- Second M.B.B.S Degree Examination, 2011: 207. Forensic MedicineDocument1 pageSecond M.B.B.S Degree Examination, 2011: 207. Forensic MedicineRadhika SethuNo ratings yet
- 4137 MCQDocument2 pages4137 MCQRadhika SethuNo ratings yet
- Second M.B.B.S Degree Examination, 2011: 204. Pathology - IiDocument2 pagesSecond M.B.B.S Degree Examination, 2011: 204. Pathology - IiRadhika SethuNo ratings yet
- 1733 MCQDocument3 pages1733 MCQRadhika SethuNo ratings yet
- Section-B: Second M.B.B.S Degree Examination, 2009Document1 pageSection-B: Second M.B.B.S Degree Examination, 2009Radhika SethuNo ratings yet
- Rishum 1 262421216 2Document1 pageRishum 1 262421216 2HellcroZNo ratings yet
- Laporan Kasus Neurogenic ShockDocument44 pagesLaporan Kasus Neurogenic ShockAkbar TaufikNo ratings yet
- Trichuris TrichiuraDocument16 pagesTrichuris TrichiuraPaul Avila SorianoNo ratings yet
- Fracture Blowout OrbitalDocument6 pagesFracture Blowout OrbitalMasitha RahmawatiNo ratings yet
- DoctorsDocument15 pagesDoctorsRitu MishraNo ratings yet
- Giotto Image3D BrochureDocument16 pagesGiotto Image3D BrochureGriselda Maria Pinto SanchezNo ratings yet
- 30613167: Management of Osteitis Pubis in Athletes Rehabilitation and Return To Training - A Review of The Most Recent Literature PDFDocument10 pages30613167: Management of Osteitis Pubis in Athletes Rehabilitation and Return To Training - A Review of The Most Recent Literature PDFRicovially DavyaNo ratings yet
- m3 Act3 Emotional DisabilitiesDocument7 pagesm3 Act3 Emotional Disabilitiesapi-516574894No ratings yet
- Daftar Harga Obat ApotekDocument7 pagesDaftar Harga Obat ApoteksalmaegaNo ratings yet
- PATHFit I Chapter 4Document6 pagesPATHFit I Chapter 4bamboogabrieltaclaNo ratings yet
- Seminar On Shock: IndexDocument37 pagesSeminar On Shock: IndexGayathri R100% (1)
- Crash CartsDocument11 pagesCrash CartsJohanna AbellanaNo ratings yet
- Management of Stroke PDFDocument6 pagesManagement of Stroke PDFtarmo angsanaNo ratings yet
- About DysphoriaDocument5 pagesAbout DysphoriaCarolina GómezNo ratings yet
- Etiology, Classification and Clinical Approach: EndophthalmitisDocument42 pagesEtiology, Classification and Clinical Approach: EndophthalmitisHieLdaJanuariaNo ratings yet
- Maternal and Early-Life Nutrition and HealthDocument4 pagesMaternal and Early-Life Nutrition and HealthTiffani_Vanessa01No ratings yet
- MCQs On IMMUNOLOGYDocument8 pagesMCQs On IMMUNOLOGYNOORNo ratings yet
- List of PG Students' Passed in May 2019 ExaminiationDocument4 pagesList of PG Students' Passed in May 2019 Examiniationyogesh kumarNo ratings yet
- Radiologia in Spondilita AnchilozantaDocument18 pagesRadiologia in Spondilita AnchilozantaMarina ApostolNo ratings yet
- Sambong UploadDocument6 pagesSambong UploadRaymond Christopher LimNo ratings yet
- Oral Biopsy: Oral Pathologist's Perspective: Review ArticleDocument7 pagesOral Biopsy: Oral Pathologist's Perspective: Review ArticleRafa LopezNo ratings yet
- Departm Ent of Education: R e P U B Lic of Tlje JH JilippineffDocument7 pagesDepartm Ent of Education: R e P U B Lic of Tlje JH JilippineffJoyce CarilloNo ratings yet
- 35 - Eposter - Subhenjit Ray.Document1 page35 - Eposter - Subhenjit Ray.Subhenjit RoyNo ratings yet
- Prevention of Venous Thromboembolic Disease in Adult Nonorthopedic Surgical Patients - UpToDateDocument54 pagesPrevention of Venous Thromboembolic Disease in Adult Nonorthopedic Surgical Patients - UpToDateSebas MontoyaNo ratings yet
- Occupy Prohibition Old Links NoteDocument52 pagesOccupy Prohibition Old Links NoteJenn DowdenNo ratings yet
- The Ultimate Guide To Strength TrainingDocument3 pagesThe Ultimate Guide To Strength Training23gomez0% (1)
- Caring For Children Receiving Chemotherapy, Antimicrobial Therapy and Long-Term Insulin TherapyDocument34 pagesCaring For Children Receiving Chemotherapy, Antimicrobial Therapy and Long-Term Insulin TherapyRubinaNo ratings yet
- Bacteriophage Therapy SummitDocument12 pagesBacteriophage Therapy SummitZhibek AbyshevaNo ratings yet
- Approach To The Adult With Epistaxis - UpToDateDocument29 pagesApproach To The Adult With Epistaxis - UpToDateAntonella Angulo CruzadoNo ratings yet