Professional Documents
Culture Documents
Bahan RAS Terapi Field
Uploaded by
Rinaldi InalCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Bahan RAS Terapi Field
Uploaded by
Rinaldi InalCopyright:
Available Formats
Aliment Pharmacol Ther 2003; 18: 949962. doi: 10.1046/j.0269-2813.2003.01782.
Review article: oral ulceration aetiopathogenesis, clinical diagnosis
and management in the gastrointestinal clinic
E. A. FIELD & R. B. A LLAN
Oral Medicine Unit, Liverpool University Dental Hospital and School, Liverpool, UK
Accepted for publication 15 August 2003
renewed interest in the role of Streptococcus sanguis and
SUMMARY
possible infectious triggering of an inappropriate immu-
Oral ulceration is a common complaint of patients noinflammatory response, resulting in tissue damage.
attending out-patient clinics. The aim of this review is to The efficacy and limitations of conventional treatment
provide the gastroenterologist with a differential for this mutisystem disorder are outlined together with
diagnosis of oral ulceration, and a practical guide for the potential role of novel biological agents, such as
the management of recurrent aphthous stomatitis, anti-tumour necrosis factor-a therapy. Oral ulceration,
including topical and systemic therapy. The association as a manifestation of inflammatory bowel disease and a
of recurrent aphthous stomatitis with Behcets disease complication of drug therapy, is described. Guidance is
and other systemic disorders, including coeliac disease, given concerning indications for referral of patients with
is discussed. Recent evidence concerning the immuno- oral ulceration to an oral physician/surgeon for further
pathogenesis of Behcets disease is reviewed, including investigations, including biopsy if appropriate.
20% of the general population at any time.3 The peak
THE DIFFERENTIAL DIAGNOSIS OF ORAL
age of RAS onset is during childhood, with a tendency
ULCERATION
to decrease in severity and frequency with age.4
The principal causes of oral ulceration are trauma,
recurrent aphthous stomatitis, microbial infections,
Clinical features
mucocutaneous disease, systemic disorders, squamous
cell carcinoma and drug therapy1, 2 (see Table 1 and Three clinical presentations of RAS are recognized:
Figures 16). minor recurrent aphthous stomatitis (MiRAS), major
recurrent aphthous stomatitis (MjRAS) and herpetiform
ulceration. The clinical presentation of these types of
RECURRENT APHTHOUS STOMATITIS
RAS are shown in Table 2.1 Patients may sometimes
Recurrent aphthous stomatitis (RAS) is characterized by present with a mixed pattern of RAS, but this is
recurrent bouts of one or several shallow, rounded or relatively uncommon.
ovoid, painful ulcers, that recur at intervals of a few
days or up to 23 months. RAS is a common oral
Minor recurrent aphthous stomatitis (MiRAS)
mucosal condition and has been reported as affecting
This is the most common form of RAS and approxi-
mately 80% of patients have lesions of this type.4 In its
Correspondence to: Dr E. A. Field, Oral Medicine Unit, Liverpool Uni-
versity Dental Hospital and School, Pembroke Place, Liverpool L3 5PS, UK. most characteristic form, MiRAS presents the picture of
E-mail: e.a.field@liv.ac.uk a number of small ulcers (one to five) appearing on the
2003 Blackwell Publishing Ltd 949
950 E. A. FIELD & R. B. ALLAN
Table 1. Principal causes of oral ulceration does not depend on the dimensions of the lesions alone,
but on a number of clinical features. The appearance of
Solitary ulcer*
Trauma the ulcer base is greyyellow, often with a red and
Squamous cell carcinoma slightly raised margin, and, unless influenced by the site
Infections (e.g. syphilis, tuberculosis) (as in the depth of the buccal sulcus where they appear
Recurrent bouts of one or more ulcers healing spontaneously elongated), they are usually oval in shape. The ulcers
Recurrent aphthous stomatitis (RAS)
are painful, particularly if the tongue is involved, and
Behcets disease
Aphthous-like ulcers due to systemic disease or drug therapy.
may make eating or speaking difficult. The course of
Recurrent erythema multiforme these ulcers varies from a few days to a little over
Single bout of ulceration, preceded by vesicles and affecting 2 weeks, but usually their duration is of the order of
multiple oral sites 10 days. Minor aphthae heal without scar formation.
Viral infections (e.g. herpangina and primary herpetic Following healing of the ulcers, there is a variable ulcer-
stomatitis)
free interval; 34 weeks is most common. In a few
Erythema multiforme
Persistent oral ulceration affecting different sites patients the recurrence of the ulcers appears to be
Mucocutaneous disease (e.g. oral lichen planus, Fig. 2) entirely random, and in some cases there may not be an
Immunobullous disease (e.g. oral pemphigus) ulcer-free period between attacks, with new aphthae
Gastrointestinal disease (e.g. Crohns disease) developing before existing ones have healed.
Haematological (e.g. leukaemia)
Drug therapy (e.g. nicorandil)
Major recurrent aphthous stomatitis (MjRAS)
* If a single persistent oral ulcer shows no sign of healing 1014 days
after any putative trauma is removed, then it must be considered as MjRAS (Figure 1) accounts for approximately 1015%
malignant, unless proven otherwise.
Patients may report intermittent oral ulceration if these conditions of cases,4 and it varies from the minor form in a number
undergo periods of remission. of important clinical features. The ulcers tend to be
larger than those of MiRAS, and they are of greater
buccal mucosa, the labial mucosa, the floor of the duration, up to a period of months in some cases.1 As a
mouth or the tongue.1 Moreover, the ulcers are usually result of the long periods of time involved, there is
concentrated in the anterior part of the mouth; the probably a tendency for the production of a heaped-up
pharynx and tonsillar fauces are rarely implicated in margin which, when a single ulcer is seen in isolation,
this form of ulceration. The prodromal stage of ulcer- may lead to the suspicion that the lesion is malignant.
ation is variable, but there is usually a sensation On eventual healing, the ulcers may leave a substantial
described as burning or prickling for a short period scar and this, together with the tissue destruction which
before the ulcers appear. Following this phase, ulcer- may occur during the active phase of ulceration, may
ation occurs directly by loss of the epithelium. The lead to gross distortion of the involved tissues. MjRAS
ulcers are usually less than 1 cm in diameter and, in may produce lesions throughout the entire oral cavity,
most instances, their size is approximately 45 mm in including the soft palate and tonsillar areas, and
diameter. However, the classification of minor RAS ulceration may extend to the oropharynx.
Table 2. Clinical features of recurrent aphthous stomatitis (RAS)
Minor (MiRAS) Major (MjRAS) Herpetiform ulceration
Peak age of onset 2nd decade 1st and 2nd decades 3rd decade
Number of ulcers/bout 15 13 520 (?100)
Size of ulcers (mm) < 10 > 10 12
Duration 714 days 2 weeks 3 months 714 days
Heal with scarring No Yes No*
Site Non-keratinized mucosa, especially Keratinized plus Non-keratinized mucosa but
labial/buccal mucosa. Dorsum nonkeratinized mucosa particularly floor of mouth and
and lateral borders of tongue. particularly soft palate. ventral surface of tongue.
* Unless a number of ulcers coalesce.
2003 Blackwell Publishing Ltd, Aliment Pharmacol Ther 18, 949962
REVIEW: ORAL ULCERATION 951
Figure 1. Major aphthous ulceration affecting the labial mucosa.
Figure 2. Ulcerative lichen planus affecting the oral mucosa.
The number of ulcers present at one time varies from last for approximately 714 days, and the period of
one to 10 in MjRAS. Frequently, a single ulcer will remission between attacks is variable. Where many
persist for a long period, while other (usually smaller) ulcers are present they may coalescence to form larger
ulcers fade. Unlike MiRAS, there does not appear to be confluent areas of ulceration, usually with marked
a cyclical pattern in MjRAS, and the ulcers are usually erythema. Healing with scar formation has been
unpredictable in their onset. Long periods of remission described in herpetiform ulceration, but this is probably
may be followed by intervals of intense ulcer activity, a result of coalescence.
without any obvious precipitating factor.1 The pro-
longed and painful ulceration may present significant
Aetiopathogenesis of RAS
problems to the patient; difficulty eating, speaking
and swallowing can severely affect a patients quality Genetic factors are likely to predispose patients to RAS,
of life. and more than 40% of affected individuals have first-
degree relatives with RAS.5 The aetiology of RAS is
unknown, but a number of predisposing factors have
Herpetiform ulceration
been implicated and include trauma, stress, smoking
This distinctive form of RAS differs in many ways from cessation, hormonal imbalance and food hypersensitiv-
both MiRAS and MjRAS, and is less common, affecting ity.1 Although some patients report that stressful life
510% of cases.4 In herpetiform ulceration the ulcers events (e.g. taking examinations in the case of students)
are small (12 mm) and multiple (as many as a can provoke an outbreak of ulcers, there is little
hundred ulcers may be present at the same time). substantive evidence to link stress to RAS.6 There
Although any nonkeratinized oral mucosa may be appears to be a negative association between smoking
involved, characteristically the affected sites are the and RAS, and some patients report the onset of oral
lateral margins of the tongue and the floor of the ulcers after smoking cessation.7 Interestingly, nicotine-
mouth. Individual ulcers are grey and without a containing tablets appear to control the frequency of
delineating erythematous border, making them quite RAS.8 Some patients report being free from aphthae
difficult to visualize: they resemble ulcers of primary whilst taking oral contraceptives or when pregnant,9
Herpes simplex virus (HSV) infection. In spite of their and a minority of women with RAS have cyclical oral
small size, these ulcers are very painful and may make ulceration related to the luteal phase of the menstrual
eating and speaking difficult. A single crop of ulcers may cycle.10 There is no convincing evidence linking
2003 Blackwell Publishing Ltd, Aliment Pharmacol Ther 18, 949962
952 E. A. FIELD & R. B. ALLAN
hypersensitivity to foods and RAS other than in coeliac are likely to share some common immunopathogenic
disease,11 but some patients recognize that foods such mechanisms the reasons why RAS lesions are confined
as chocolate, cheese and tomatoes can precipitate to the oral cavity, and the oral lesions in Behcets
attacks of RAS. disease are associated with multisystem disease remains
There is strong evidence from histopathological and unclear.16
immunological studies that T-cell-mediated immune
responses are implicated in RAS.1113 Three stages are
Systemic conditions and aphthous-like lesions
recognized in the development of an aphthous ulcer.12
Microscopic examination during the pre-ulcerative Table 3 lists the principal systemic conditions associated
stage reveals a mononuclear (lymphocytic) cell infiltrate with aphthous-like ulcers. These frequently start in
in the epithelium focal vacuolation and is followed by adulthood with no previous history of oral ulceration.
degeneration of the suprabasal epithelial cells accom-
panied by a mononuclear, mainly lymphocytic infiltrate
Gastrointestinal disorders
in the lamina propria. As the ulcerative stage approa-
ches there is increased infiltration of the tissues, Crohns disease and ulcerative colitis may occasionally
particularly the epithelium, by mononuclear cells and be associated with RAS20 but are more likely to manifest
accompanied by more extensive oedema and degener- as other types of oral ulceration. The association of RAS
ation of the epithelium progressing to frank ulceration with coeliac disease is well established. A number of
with a fibrinous membrane covering the ulcer. During studies have suggested up to 5% of out-patients who
the healing phase there is regeneration of the epithe- initially present with RAS11, 21, 22 have gluten-sensitive
lium. The immunopathogenesis of RAS has yet to be enteropathy (GSE). These RAS patients may not always
fully elucidated, but the infiltration of the epithelium by have gastrointestinal symptoms or other clinical fea-
T lymphocytes is likely to be in response to some, as yet tures of coeliac disease but usually have folate deficiency
unidentified, keratinocyte-associated antigen. Keratino- and sometimes reticulin antibodies,21 particularly
cyte death is thought to be mediated by the differentiation immunoglobulin-A-class reticulin and/or gliaden anti-
of cytotoxic T cells and involves the production of tuour bodies.23 A recent study has demonstrated that the
necrosis factor-a (TNFa) by these and other leuco- prevalence of RAS in a population with coeliac disease
cytes.14 TNFa induces inflammation by its effect on did not significantly differ from an unaffected matched
endothelial cell adhesion and neutrophil chemotaxis.14 population without coeliac disease. The authors con-
Other cytokines, e.g. interleukin and interleukin-2, may clude therefore that coeliac disease should be referred to
also play a role in the immunopathogenesis of RAS.15 as a risk indicator not a risk factor for RAS.24 A high
Oral streptococci were previously suggested as import- prevalence of HLA-DRW10 and DQW1 has been
ant in the pathogenesis of RAS and Behcets disease, associated with RAS.25 RAS in patients with coeliac
either as direct pathogens or an antigenic stimulus, disease appears to remit completely on a gluten-free
culminating in the genesis of antibodies that may diet;26 however, there is conflicting evidence concern-
conceivably cross-react with keratinocyte antigenic ing the remission of RAS in patients without GSE, who
determinants.16 More recently a common antigen was undergo dietary withdrawal of gluten. There may be a
demonstrated between oral mucosa and the 65 kDa few RAS patients, with no detectable clinical or
heat shock protein (HSP). As there is a high degree of histological evidence on jejunal biopsy, who may
homology between the microbial 65 kDa and human
60 kDa HSP, the hypothesis was suggested that an Table 3. Systemic conditions and aphthous-like lesions
autoimmune response to the endogenous HSP might be
Behcets disease
responsible for the pathological changes in Behcets
Nutritional deficiencies
disease.17 The role of the cd T-cell subset in the Gastrointestinal disorders
immunopathology of RAS and Behcets disease and Cyclical neutropenia
their participation in the immune response to bacteria- HIV infection
derived and autologous antigens in these conditions is MAGIC syndrome
FAPA syndrome
currently under investigation (see section on Behcets
Drug reactions
disease).13, 18, 19 Although RAS and Behcets disease
2003 Blackwell Publishing Ltd, Aliment Pharmacol Ther 18, 949962
REVIEW: ORAL ULCERATION 953
respond to a gluten-free diet,27, 28 but a study by tinic deficiency. This includes a full blood count and
Hunter et al.29 showed no significant benefit for RAS film, and measurement of inflammatory markers and
patients without evidence of coeliac disease. haematinics (serum ferritin, serum B12, serum and red
cell folate). If there is any suspicion of coeliac disease,
either due to the patients history or evidence of
Other systemic conditions and factors
malabsorption on routine testing, then serological
Haematinic deficiencies (iron, folic acid or vitamin B12) testing for anti-endomysial antibody and other appro-
have been reported to be twice as common in RAS priate investigations should be undertaken: is debatable
patients than in controls.16 One US study, however, did whether all RAS patients should undergo screening for
not report any iron or folic acid deficiency in RAS coeliac disease. Table 4 lists some of the therapeutic
patients,30 and there is no convincing evidence of B6 or options available for the management of patients with
zinc deficiency in individuals with RAS. Replacement RAS.1 The choice of therapy for RAS depends on the
therapy has not met with uniform success, although severity and frequency of ulceration, but the objectives
RAS may improve in some patients who are nutrition- of treatment are to relieve discomfort, reduce secondary
ally deficient.31 HIV-associated ulcers tend to occur in infection, promote healing of existing ulceration and
crops of five or less on nonkeratinized mucosa, and may prevent new ulcers occurring.
resemble minor or major aphthae. The ulcers are Topical analgesic sprays or rinses such as benzydamine
frequently very painful and last for several months; hydrochloride can be used to reduce discomfort; how-
they can be extremely debilitating in these patients and ever, 2% lignocaine (lidocaine) gel, diluted as a rinse, is
can cause problems with eating. Care must be taken to more effective for severe cases of RAS. Care must be
exclude HSV or cytomegalovirus infection in HIV- taken if used in the posterior part of the mouth, as
infected patients presenting with oral ulceration. Large stronger analgesic preparations can affect the laryngeal
major-aphthous-type ulcers are likely to be seen in HIV reflexes: long-term use of topical lignocaine (lidocaine)
patients with low CD4T lymphocyte counts.32, 33 It has
been postulated that the immune imbalance associated
with HIV disease may amplify the local breakdown in Table 4. Therapeutic options for recurrent aphthous stomatitis
immunoregulation in RAS and lead to more severe (RAS)1
ulcers.33 A significant number of patients with cyclical
Topical antiseptic Chlorhexidine gluconate (mouthwash)
neutropenia present with aphthous-type ulceration
Topical analgesics: Benzydamine hydrochloride
which occurs at intervals (often monthly), reflecting (mouthwash)
their neutropenic status.16 Patients who are function- Lignocaine (lignocaine (lidocaine)) rinse
ally neutropenic, for example those with chronic Topical corticosteroids: Hydrocortisone hemisuccinate (pellets)
granulomatous disease or benign familial neutrope- Triamcinolone acetonide
nia,34 are also susceptible to aphthous-type ulcer- (in adhesive paste)
Betamethasone valerate (mouthwash)
ation.35 Other systemic conditions associated with this Beclometasone dipropionate (spray)
type of ulcer include MAGIC (mouth and genital ulcers Budesonide (spray)
with inflamed cartilage) syndrome36 FAPA (periodic Triamcinolone (with or without
fever, aphthous ulcers, pharyngitis and cervical adeni- chlortetracycline) mouthwash
tis) syndrome,37 and Sweets syndrome.38 Topical antibiotic: Chlortetracycline mouthwash
Systemic Prednisolone
immunomodulators: Azathioprine
Management of RAS Colchicine
Ciclosporin
The diagnosis of RAS is not usually difficult and may be Thalidomide
deduced, in most cases, from the history and charac- Other therapies that have been advocated
teristic clinical appearance. If there is any doubt about Cimetedine Low-energy laser
the diagnosis then appropriate diagnostic tests should Carbenoxolone Levamisole
be arranged to exclude other causes of oral ulceration. 5-Aminosalicylic acid Nicotine
Dapsone Interferon-a
Patients with persistent and troublesome RAS should
Pentoxphylline Sucralfate
undergo screening to check for an underlying haema-
2003 Blackwell Publishing Ltd, Aliment Pharmacol Ther 18, 949962
954 E. A. FIELD & R. B. ALLAN
is not advisable, as it may be absorbed. Several pastes times daily) is adhered to. In severe MiRAS unrespon-
and gels can be used to coat the surface of the ulcers sive to these preparations and in MjRAS it may be
and form a protective barrier against secondary infec- necessary to use a more potent steroid preparation1
tion and further mechanical irritation. Some difficulty such as a betamethasone sodium phosphate rinse
may be experienced in applying some of these prepara- (dissolve 0.5 mg in 5 mL of water and rinse for
tions, particularly to large ulcers and to those at the 23 min), steroid aerosol (e.g. beclometasone dipropr-
back of the mouth. Antiseptic mouthwashes containing ionate, 100 lg/puff), or a high-potency topical cortico-
chlorhexidine are widely used for the symptomatic steroid, such as clobetasol 0.05% in orabase (1 : 1) or
treatment of RAS and are considered helpful by many fluocinonide 0.05% in orabase (1 : 1).39 Prolonged use
patients, particularly if oral hygiene is difficult to of potent topical corticosteroids carries a risk of systemic
maintain because of oral ulceration. Extrinsic staining absorption and associated adverse effects; it may also
of teeth associated with long-term use of chlorhexidine predispose to oral candidosis.
may be a problem. A more effective measure in the relief In severe cases of RAS, particularly MjRAS, it may be
of symptoms caused by secondary infection is the necessary to use some form of systemic therapy
application of topical antibiotics. A mouthwash contain- (Table 4); however, all drugs have side-effects and risks
ing tetracycline (dissolve soluble tetracycline capsule which must be weighed against their benefits for RAS.
250 mg in 510 mL water and rinse) or chlortetracy- Apart from prednisolone, a number of systemic drug
cline is often highly effective in reducing the pain therapies has been advocated for the treatment of
caused by severe ulceration, and as a result of the much MjRAS and in some cases Behcets disease. Thalidomide
less heavily colonized environment the ulcers often heal has been used successfully for severe RAS which has
more rapidly than otherwise. The treatment of herpe- failed to respond to other treatment modalities; it has
tiform ulceration depends largely on this therapy, and also been advocated for use in HIV-associated oral
response to the antibiotic mouthwash is often rapid and ulceration.4 Thalidomide is a TNFa inhibitor that has
complete. There are obvious disadvantages, however, in anti-inflammatory effects; however, its use is limited
the use of broad-spectrum antibiotics for this purpose, because of teratogenic and other adverse effects
the risk of hypersensitivity reactions and the encour- (e.g. irreversible polyneuropathy). The potential use
agement of growth of resistant organisms being the of anti-TNF therapy by novel biological agents
most important. Local secondary infection by oppor- (e.g. infliximab) for recurrent aphthae in Behcets
tunists such as Candida species may be a problem and disease is discussed in the next section. Colchicine inhib-
limits long-term use. its cell-mediated immune responses and has been used
Topical corticosteroids can be effective drugs in the in does of 1.51.8 mg/day successfully in two small,
treatment of RAS. Patient response is variable, and open studies involving 23 patients with RAS.40, 41
there are some individuals who gain little or no relief
from their use. Corticosteroids used in this manner have
BEHC ETS DISEASE
two modes of action; their anti-inflammatory action
modifies, in a minor way, the progress of the ulceration Behcets disease is a multisystem, chronic relapsing
at all stages and to some extent reduces the discomfort inflammatory disease of unknown cause, which is
experienced. The second effect of steroids, i.e. the specific characterized by recurrent oral (aphthous) ulcers,
blocking effect of the T lymphocyte ) epithelial cell genital ulcers, uveitis and skin lesions.42 There may
interaction, is much more important in the present be a variety of other manifestations including joint,
context. Since the concentration of sensitized lympho- central nervous system, vascular and intestinal lesions
cytes occurs before and during the early stages of oral of variable severity.42
ulceration, it follows that the drugs exert their maxi- In 1990 the International Study Group for Behcets
mum effect at this time. The drugs most commonly disease proposed criteria for the diagnosis of the disease
adopted for local oral application in RAS are hydrocor- (Table 5).43 According to these criteria, RAS must be
tisone hemisuccinate (as pellets of 2.5 mg) and triam- present as well as at least two of the following: recurrent
cinolone acetonide (in an adhesive paste containing genital ulceration, eye lesions, skin lesions and a
0.1% of the steroid). There is little risk of adrenal positive pathergy test. Behcets disease has diverse
suppression provided that the recommended dose (four clinical manifestations and lacks any pathognomonic
2003 Blackwell Publishing Ltd, Aliment Pharmacol Ther 18, 949962
REVIEW: ORAL ULCERATION 955
Table 5. International Study Group for
Manifestations Prevalence (%) Description
Behcets Disease (ISGBD): Criteria for diag-
nosis of Behcets disease43 Recurrent oral 100 Minor aphthous.
ulceration Major aphthous or herpetiform ulceration
observed by a physician or reported
reliably by patient.
Recurrent at least three times in one
12-month period.
Plus two of:
Recurrent genital 80 Recurrent genital aphthous ulceration
ulceration or scarring, especially in male patients,
observed by physician or reliably reported
by patient.
Eye lesions 6070 Anterior uveitis.
Posterior uveitis.
Cells in vitreous on slit lamp examination.
Or
Retinal vasculitis observed by qualified
physician (ophthalmologist)
Skin lesions 6080 Erythema nodosum-like lesions observed
by physician or reliably reported by patient.
Pseudofolliculitis.
Papulopustular lesions.
Or
Acneiform nodules consistent with Behcets
disease observed by physician and in
post-adolescent patients not receiving
corticosteroids
Positive pathergy Variable An erythematous papule, > 2 mm, at the prick
test 48 h after the application of sterile needle,
2022 gauge, which obliquely penetrated
avascular skin to a depth of 5 mm;
read by a physician at 48 h.
symptoms or diagnostic laboratory markers: conse- onset or family history. Scrutiny of clinical photo-
quently it is often difficult to diagnose. graphs taken of Behcets disease patients in this study
suggested that both herpetiform-type and aphthous-
type ulcers appeared atypical.44 Clinical observations
Oral ulceration in Behcets disease
in oral medicine clinics suggest that aphthous ulcers in
RAS is seen in all patients with Behcets disease; it patients with Behcets disease appear to be associated
commonly precedes other systemic features and can be with increased tissue oedema and appear to have an
of major, minor or herpetiform types. However, it is intensely erythematous border. The aphthae in
difficult to predict with any certainty those patients Behcets disease often occur in the soft palate and
initially presenting with RAS who will subsequently oropharynx and have been observed on the hard
proceed to develop multisystem involvement as part of palate, which is an unusual site for RAS in patients
Behcets disease. Two studies have addressed this without Behcets disease.44 Patches of mucosal ery-
problem; in one, a clinical comparison between 38 thema may be observed in patients with the disease,
patients with Behcets disease and RAS-only controls indicating possible instability of the oral mucosa prior
showed an increased number of concurrent ulcers and to ulceration. Patients may paradoxically report no
involvement of the soft palate and oropharynx in those painful symptoms during active disease, despite exten-
diagnosed with Behcets disease.44 No differences were sive oral ulceration being clinically evident. A Korean
detected with respect to duration, frequency, age of study examined the prognosis of the clinical relevance
2003 Blackwell Publishing Ltd, Aliment Pharmacol Ther 18, 949962
956 E. A. FIELD & R. B. ALLAN
of recurrent oral ulceration in Behcets disease, and antigens.19 cd T Cells have also been reported as
investigators found that approximately half the producing several cytokines, with the cytokine profile
patients who were initially diagnosed as RAS-only dependent on the nature of antigen, enabling the cd
developed other manifestations of Behcets disease at T cells to influence the nature of the immune
an average of 7.7 years after onset.45 Highly recurrent response.50 Levels of circulating TNFa, interleukin-
RAS appeared to be a warning signal for Behcets 1-b and interleukin-8 have been reported as elevated
disease in this study.45 in Behcets disease, and it has been postulated that
these cytokines may be involved in the activation of
neutrophils.51 Bank et al. have recently demonstrated
Aetiopathogenesis of Behcets disease
and substantiated data from a number of other studies
The aetiology of Behcets disease is poorly understood, indicating that cd T cells have increased in Behcets
but interactions between environmental and genetic disease relative to healthy and disease controls, and in
factors are likely to influence the susceptibility and addition the cd T-cell population increases with the
development of the disease,46 as well as being impli- active disease.19 This group also examined the prolif-
cated in its pathogenesis. Susceptibility to Behcets eration of a subset of cd T cells in response to bacterial
disease is associated with the HLA-B51 MHC class 1 products obtained from patients with the active
allele, and it has been reported that individuals in the mucocutaneous disease, and concluded that an exag-
appropriate geographical setting (i.e. living in areas gerated proliferative response to products released by
along the Silk Route) who express this allele have an micro-organisms present in oral (aphthous) ulcers may
eight- to ten-fold greater risk of developing the play a role in the expansion of cd T cells in Behcets
disease.42 The relative risk of the disease among disease.19 This raises the possibility that therapeutic
carriers of HLA-B5I is much less in Western countries, control of the oral environment, or manipulation of
indicating that other genetic factors may be important cd T-cell-derived cytokines by drugs such as anti-
in these individuals.42 The HLA-51 allele also affects TNFa, provides effective strategies against aphthous
the severity of Behcets disease, since it is more ulceration and thereby controls systemic manifesta-
commonly detected in patients with posterior uveitis tions of the disease.48
or progressive central nervous system disease than
those with milder disease.42 Investigation of the
Treatment of Behcets disease
aetiology of Behcets disease has focused predomin-
antly on herpes simplex virus immunopathology, Patients with Behcets disease usually have repeated
autoimmunity to oral mucosa or cross-reactive micro- exacerbations and remission of their clinical symptoms,
bial antigens, and streptococcal infection.47 Its im- and in these individuals treatment is essentially symp-
munopathogenesis is likely to involve a T-cell-mediated tomatic. The choice of therapy depends on whether the
response, and it has been demonstrated that lympho- clinical manifestations of the disease are local or
cyte function is abnormal in patients with the systemic. Multidisciplinary involvement in the manage-
disease.13 There has been renewed interest in the role ment of Behcets disease is essential, and patients should
of Streptococcus sanguis as a causative agent,48 and ideally be treated in centres with extensive experience of
recent advances have resurrected the theory of infec- treating the disease.
tious triggering of the immune cascade in Behcets Local treatment with corticosteroids often controls oral
disease and have been strengthened by work with and genital ulcers, and immunosuppressive therapy is
heat-shock protein and the concept of a molecular reserved for severe cases of mucocutaneous involve-
mimicry mechanism.49 It has been suggested that ment.52 The oral lesions may respond well to topical
bacterial products such as heat-shock proteins corticosteroid preparations (Table 4), but it is important
may incite an inappropriate immunoinflammatory to monitor the patients for signs or oral candidosis and
response.19 Recent studies have investigated the role treat this with appropriate antifungal agents. Patients
of the cd T-cell subset in the immunopathology of with painful oral ulceration also benefit from analgesic
Behcets disease.13, 18, 19 These T cells participate in mouthwashes, e.g. benzydamine hydrochloride or ligno-
the immune response to infections and in autoimmu- caine (lidocaine). The choice of systemic drug treatment
nity by recognizing bacteria-derived and autologous for Behcets disease is dictated by the patients clinical
2003 Blackwell Publishing Ltd, Aliment Pharmacol Ther 18, 949962
REVIEW: ORAL ULCERATION 957
manifestations, but conventional therapy relies on anti-
ORAL ULCERATION AND INFLAMMATORY
inflammatory and immunomodulatory agents. There is
BOWEL DISEASE
a paucity of controlled clinical trails relating to drug
therapy, and prescribing for Behcets disease is, to a Oral involvement has for some time been recognized in
large extent, empirical.53 Ocular lesions in Behcets patients suffering from both Crohns disease and, to a
disease must be vigorously treated to prevent blindness, lesser extent, ulcerative colitis. Oral lesions may precede
and therapy aims to reduce both the severity and or accompany gastrointestinal disease and can be the
frequency of ocular attacks. Despite therapeutic inter- only site of involvement.
ventions, approximately 25% of all patients with ocular
manifestations of Behcets disease will become blind.54
Oral Crohns disease and orofacial granulatosis (OFG)
Systemic corticosteroids continue to be used extensively,
and may be administered as intravenous pulse therapy. Over the last decade there has been increasing attention
Ciclosporin is highly effective for ocular lesions, partic- paid to noninfectious granulomatous disorders of the
ularly in cases that have been refractory to other orofacial region, which include oral Crohns disease and
therapies, but its nephrotoxity restricts usage of the oral sarcoid, as well as clinical entities, known as the
drug.54 Azathioprine is a disease-modifying drug for MelkerssonRosenthal syndrome, and Miescheners
Behcets disease and helps reduce recurrences; it is now cheilitis granulomatosa (granulomatous cheilitis). The
considered to be the first-line drug for this condition. term orofacial granulomatosis (OFG) was introduced to
Thalidomide, despite its prescribing limitations and encompass these disorders and to describe a clinical
neurotoxic side-effects, has proved effective for the syndrome presenting with swelling of the face, lips or oral
management of mucocutaneous lesions in Behcets tissues in association with histological evidence of noncea-
disease56 but it is not disease-modifying, and with- seating granulomatous inflammation within these tis-
drawal of the drug can lead to severe rebound of sues.63 Recent studies have investigated the association of
symptoms.57 After teratogenicity, polyneuropathy is the OFG with intolerance to specific foods, food additives,
second most serious complication of thalidomide, and flavouring and the constituents of toothpastes. Cinnamon-
has been reported in up to 50% of patients taking the aldehyde and sodium benzoates have been particularly
drug.58 Thalidomide-related polyneuropathy appears to implicated in this respect, and in some series there was a
be dose-related and can be irreversible if not diagnosed clinical response to specific elimination diets. It remains
early. Mycophenolate mofetil does not appear to be unknown whether sensitivity to food additives is the
effective for Behcets disease.59 Colchicine is frequently primary factor for some patients with OFG or a secondary
used, and recent trials have demonstrated its beneficial aggravating factor to some underlying process.64, 65
effects on mucocutaneous symptoms, presumably by The prevalence of OFG has not been determined but
inhibiting neutrophil function.60 Cyclophosphamide, there does seem to be a geographical variation, for
with or without corticosteroids, may be indicated for example the west of Scotland, UK, appears to have a
central nervous system lesions.42, 52 higher number of cases.66 Oral medicine centres
Recognition of the possible pathogenetic role of TNFa throughout the UK are reporting an increased number
in Behcets disease has resulted in the use of anti-TNFa of cases of OFG, but this may be a result of increasing
therapy. Recent trials with novel anti-TNFa agents awareness and/or reporting of this condition. One study
(infliximab and etenercept)61 have indicated effective of 60 patients has reported that the median age of OFG
short-term remission. Infliximab (a chimeric anti-TNFa at presentation was 20 years,63 but clinical experience
monoclonal antibody) has been used successfully for the indicates that many patients are older children or
treatment of recalcitrant orogenital ulceration in Be- teenagers. The association of OFG with Crohns disease
hcets disease.62 These novel biological agents are, elsewhere in the gut has been the subject of debate, and
however, expensive compared with conventional treat- this inter-relationship has been fully explored in a
ment, and their long-term efficacy is yet to be proven in number of studies.67 The prevalence of symptomless
clinical trials. Overall, the goal of management in intestinal disease of Crohns in patients with OFG has
Behcets disease is to treat early to improve morbidity, to been reported as between 10% and 48% in various
avoid recurrences and irreversible damage to organs,57 studies.67 The clinical features of OFG are shown in
and to provide symptomatic relief for patients. Table 6.
2003 Blackwell Publishing Ltd, Aliment Pharmacol Ther 18, 949962
958 E. A. FIELD & R. B. ALLAN
Table 6. Clinical features of orofacial granulomatosis67
Swelling of lips and face*
Mucosal tags or cobblestoning
Oral ulceration (RAS and non-RAS)
Angular cheilitis
Lip fissures
Persistent lymphadenopathy
Peri-oral erythema and scaling of skin
Full-width gingivitis
* Fissured tongue (lingua plicata) and facial palsy are other manifes-
tations of the MelkersonRosenthal syndrome.
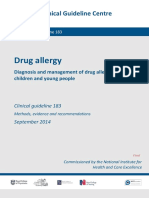
Oral ulceration and orofacial granulomatosis. Oral ulcer-
ation can be a particularly troublesome feature of
OFG, and persistent linear ulcers (non-RAS) tend to
occur at the base of hyperplastic tissue folds, partic-
ularly in the buccal and labial sulci, and can be
painful, particularly when eating (Figure 3). A thick-
ened buccal mucosa can also become traumatized
Figure 4. Pyostomatitis vegetans manifesting as snail-track
along the occlusal ridge, resulting in ulceration; this ulcers on the gingivae.
can be quite deep and may become secondarily
infected. Patients may also present with RAS, but
this is not specific to OFG. should be carried out by an experienced operator.
Histologically, noncaseating and epithelioid granulo-
Management of orofacial granulomatosis. Patients with mas, with or without multinucleated giant cells, are
OFG must be appropriately investigated, not only to seen in about 90% of cases. Granulomas are not always
confirm the diagnosis but to identify any provoking present, and their absence does not exclude the clinical
factors and signs and symptoms suggestive of an diagnosis of OFG. Granulomata may only be present in
underlying systemic condition, such as Crohns disease the underlying muscle, and it is therefore advisable to
or sarcoidosis. Biopsy of an affected site (usually the extend the biopsy deeper beyond the superficial tissue.
labial or buccal mucosa and occasionally the gingivae) Whether or not all patients with OFG should be patch-
tested to identify possible allergies to foods, or food
additives, is debatable. To date there is no totally
convincing evidence of a clinical response to elimination
diets, but there may be a therapeutic role for dietary
manipulation in some patients. If OFG presents as a
manifestation of underlying Crohns disease or sarcoi-
dosis then this must be appropriately managed. Symp-
tomatic therapy for associated oral ulceration and RAS
includes the use of topical steroids (Table 4) together
with antiseptic and analgesic mouthwashes. A large
number of systemic drugs have been used for OFG.
Short reducing courses of prednisolone may be helpful
for severe oral ulceration, but long-term steroids are
contra-indicated, particularly as many affected individ-
uals are children or teenagers. Azathioprine has proved
to be effective in some cases of OFG; other drugs advo-
Figure 3. Linear ulceration in the labial sulcus of a patient with cated for this condition include clofazimine, hydroxy-
oral Crohns disease. chloroquine, danazol, cyclosporin, sulazosulfapyridine,
2003 Blackwell Publishing Ltd, Aliment Pharmacol Ther 18, 949962
REVIEW: ORAL ULCERATION 959
thalidomide, tacrolimus and antimicrobials, such as Other types of oral ulceration have been described in
metronidazole and cotrimoxazole.67 Overall, results of patients with inflammatory bowel disease; pyostomatitis
drug therapy for OFG and its associated oral ulceration gangrenosum is rare but manifests as deep, foul-
are disappointing and unpredictable.67 smelling ulceration (Figure 5) with an irregular outline
and rolled margins.71, 72
Pyostomatitis and inflammatory bowel disease
DRUG-INDUCED ORAL ULCERATION
Pyostomatitis vegetans is a rare oral disorder that is
consistently associated with chronic inflammatory Oral ulceration is a well recognized but under-appreciated
bowel disease and considered to be a highly specific adverse drug reaction produced by or implicated in a
marker for inflammatory bowel disease.67 The bowel number of prescribed and over-the-counter medications.73
symptoms often precede oral involvement by several The underlying mechanism in drug-induced oral ulcer-
months or years. Pyostomatitis vegetans has a distinct ation is often unclear, but it can be due to local application
clinical appearance with miliary abscesses and pustular of irritant preparations, such as aspirin74 and pancreatic
lesions affecting the oral mucosa and gingiva, which supplements,75 or the effects of systemic drugs.2 Patients
become thickened, erythematous and may exhibit with learning disabilities or the elderly may have difficulty
vegetations or cobblestoning.68 Pustular lesions often swallowing medication or may hold medication in the
rupture, leading to erosions and ulceration, with mouth, referred to as pouching, increasing the contact
fissuring, in a pattern described as snail-track ulcer- time of medication in localized areas.76
ation.69 The oral lesions predominantly affect the labial A wide spectrum of systemic drugs has been implicated
and buccal mucosa and the labial attached gingivae as causing oral ulceration,2 with clinical presentations
(Figure 5), although the hard and soft palate, vestibule ranging from superficial, nonspecific ulceration to
and tonsillar region can also be affected. The histological aphthous-like lesions or widespread erosions of the
features of pyostomatitis vegetans are often character- mucosa.2 Aphthous-like and nonspecific oral ulceration
istic, although not pathogenomonic, showing intraepit- may be caused by nicorandil (potassium channel
helial and subepithelial microabscesses containing large activator), captopril77 and some nonsteroidal anti-
numbers of eosinophils. Topical steroid therapy has been inflammatory drugs,78 but the exact pathogenic mech-
successful for the treatment of pyostomatitis vegetans, anisms remain unclear.2 There are increasing reports of
but in many cases systemic treatment, with or without nicorandil-induced oral ulceration (Figure 6),79 and in
azathiopine or sulfamethoxypyridazine, is required.70 one report of six cases from European centres, severe oral
Management of the associated inflammatory bowel ulceration appeared within 110 months of starting
disease may result in improvement of the oral lesions. nicorandil and mostly involved the tongue (Figure 6)
Figure 5. Pyostomatitis gangrenosum: ulceration on the dorsum Figure 6. Non-specific oral ulceration on the tongue, in a patient
of the tongue. taking nicorandil.
2003 Blackwell Publishing Ltd, Aliment Pharmacol Ther 18, 949962
960 E. A. FIELD & R. B. ALLAN
and buccal mucosa.80 Analysis of another six cases should be referred to an oral physician/surgeon for
suggested that a threshold dosage of 30 mg/day of further investigations, including biopsy if appropriate.
nicorandil might be necessary to induce the aphthous-
like lesions.81 Drugs used to suppress rheumatic dis-
ACKNOWLEDGEMENT
eases have been reported as causing oral ulceration, and
include penicillamine,82 gold75 and methotrexate.83 A We acknowledge the expert advice of Professor Farida
number of chemotherapeutic agents cause severe dis- Fortune BDS, FDSRCS, MB BS, FRCP, Professor of
comfort due to oral ulceration, and widespread mucosal Medicine in relation to Oral Health, Barts and the
involvement may necessitate opioid therapy or alter- Royal London, Queen Marys School of Medicine and
ation to the therapeutic regimen.84 Opportunistic infec- Dentistry, concerning Behcets disease.
tions secondary to cytoxic chemotherapy can also
manifest as oral ulceration.2 Patients who develop
REFERENCES
lichenoid-drug eruptions affecting the mouth may report
persistent or intermittent oral ulceration, and a wide 1 Field EA, Longman LP. Tyldesleys Oral Medicine, 5th edn.
range of systemic drugs have been implicated in this Oxford: Oxford University Press, 2003.
2 Porter SR, Scully C. Adverse drug reactions in the mouth. Clin
adverse reaction.2 A detailed list of current medications
Dermatol 2000; 18: 52532.
is critical to identify drug-induced oral ulceration, 3 Rennie JS, Reade PC, Hay KD, et al. Recurrent aphthous sto-
especially when the ulceration is resistant to therapy matitis. Br Dent J 1985; 159: 3617.
and of indeterminate cause.77 It is important to ascertain 4 Rogers RS, 3rd. Recurrent aphthous stomatitis. Clinical
if the oral ulceration started, or became worse, at the characteristics and associated systemic disorders. Semin
Cutan Med Surg 1997; 16: 27883.
commencement of drug therapy or after an increased
5 Shohat-Zabarski R, Kalderon S, Klein T, et al. Close association
dosage. Patients with drug-induced oral ulceration may of HLA-B51 in persons with recurrent aphthous stomatitis.
show improvement with topical corticosteroid treat- Oral Surg Oral Med Oral Pathol 1992; 74: 4558.
ment, but definitive management is dependent on 6 Pedersen A. Psychologic stress and recurrent aphthous
withdrawal of the putative drug; occasionally this is ulceration. J Oral Pathol Med 1989; 18: 11922.
not an option. Older patients especially, but not exclu- 7 Dorsey C. More observations on relief of aphthous stomatitis
on resumption of cigarette smoking. Calif Med 1964; 101:
sively, may be taking multiple medications, a number of
3778.
which have been implicated as causing oral ulceration; 8 Bittoun R. Recurrent aphthous ulcers and nicotine. Med J
this poses difficult and challenging management. Aust 1991; 154: 4712.
9 Ferguson MM, McKay Hart D, et al. Progeston therapy for
menstrually related aphthae. Int J Oral Surg 1978; 7: 46370.
CONCLUSION 10 Ferguson MM, Carter J, Boyle P. An epidemiological study of
factors associated with recurrent aphthae in women. J Oral
All patients with recurrent or persistent oral ulceration Med 1984; 39: 2127.
should be fully investigated to establish a definitive 11 Ferguson MM, Wray D, Carmichael HA, et al. Coeliac disease
diagnosis and eliminate the possibility of an underlying associated with recurrent aphthae. Gut 1980; 21: 2236.
systemic disorder or oral malignancy. The diagnosis of 12 Soames JV, Southam JC. Oral Pathology, 3rd edn. Oxford:
RAS is based on the patients history and clinical Oxford University Press, 1998.
13 Freysdottir J, Lau S, Fortune F. Gammadelta T cells in Behcets
appearance of the ulcers. The majority of RAS cases
disease (BD) and recurrent aphthous stomatitis (RAS). Clin
respond to topical corticosteroid and/or topical antimi- Exp Immunol 1999; 118: 4517.
crobial therapy, but a few will require systemic 14 Natah SS, Hayrinen-Immonen R, Hietanen J, et al. Immuno-
immunomodulators. Patients with RAS may proceed localisation of tumour necrosis factor-alpha expressing cells in
to develop Behcets disease, which is diagnosed solely on recurrent aphthous ulcer lesions (RAU). J Oral Pathol Med
2000; 29: 1925.
the basis of clinical criteria. In spite of recent advances
15 Sun A, Chu CT, Liu BY, et al. Expression of interleukin-2
in systemic therapy for Behcets disease the functional receptor by activated peripheral blood lymphocytes upregu-
prognosis of patients will remain poor until the lated by the plasma level of interleukin-2 in patients with
underlying pathogenesis of the disease is elucidated. recurrent aphthous ulcers. Proc Natl Sci Counc Repub China
Clinical trials are currently being conducted to investi- B 2000; 24: 11622.
gate the efficacy of anti-TNFa. agents for Behcets 16 Porter SR, Scully C, Pedersen A. Recurrent aphthous stoma-
titis. Crit Rev Oral Biol Med 1998; 9: 30621.
disease. Patients with undiagnosed oral ulceration
2003 Blackwell Publishing Ltd, Aliment Pharmacol Ther 18, 949962
REVIEW: ORAL ULCERATION 961
17 Lehner T, Lavery E, Smith R et al. Association between the 35 Wright DG, Dale DC, Fauci AS, et al. Human cyclic neu-
65-kilodalton heat shock protein, Streptococcus sanguis, and tropenia: clinical review and long-term follow-up of patients.
the corresponding antibodies in Behcets syndrome. Infect Medicine (Baltimore) 1981; 60: 113.
Immunol 1991; 59(4): 143441. 36 Orme RL, Nordlund JJ, Barich L, et al. The MAGIC syndrome
18 Hasan A, Fortune F, Wilson A, et al. Role of gamma delta (mouth and genital ulcers with inflamed cartilage). Arch
T cells in pathogenesis and diagnosis of Behcets disease. Dermatol 1990; 126: 9404.
Lancet 1996; 347: 78994. 37 Marshall GS, Edwards KM, Butler J, et al. Syndrome of periodic
19 Bank I, Duvdevani M, Livneh A. Expansion of gammadelta fever, pharyngitis and aphthous stomatitis. J Pediatr 1987;
T-cells in Behcets disease: role of disease activity and micro- 110: 436.
bial flora in oral ulcers. J Labor Clin Med 2003; 141: 3340. 38 Notani K, Kobayashi S, Kondoh K, et al. A case of Sweets
20 Veloso FT, Carvalho J, Magro F. Immune-related systemic syndrome (acute febrile neutrophilic dermatosis) with palatal
manifestations of inflammatory bowel disease: a prospective ulceration. Oral Surg Oral Med Oral Pathol Oral Radiol Endod
study of 792 patients. J Clin Gastroenterol 1996; 23: 2934. 2000; 89: 4779.
21 Ferguson R, Basu MK, Asquith P, et al. Jejunal mucosal 39 Lozada-Nur F, Miranda C, Maliksi R. Double-blind clinical trial
abnormalities in patients with recurrent aphthous ulceration. of 0.05% clobetasol propionate ointment in orobase and
Br Med J 1976; 1: 113. 0.05% fluocinonide ointment in orobase in the treatment of
22 Veloso FT, Saleiro JV. Small-bowel changes in recurrent patients with oral vesiculoerosive diseases. Oral Surg Oral Med
ulceration of the mouth. Hepatogastroenterology 1987; 34: Oral Pathol 1994; 77: 598604.
367. 40 Katz J, Langevitz P, Shemer J, et al. Prevention of recurrent
23 Merchant NE, Ferguson MM, Ali A, et al. The detection of IgA- aphthous stomatitis with colchicine: an open trial. J Am Acad
reticulin antibodies and their incidence in patients with Dermatol 1994; 31: 45961.
recurrent aphthae. J Oral Med 1986; 41: 314. 41 Gatot A, Tovi F. Colchicine therapy in recurrent oral ulcers.
24 Sedghizadeh PP, Shuler CF, Allen CM, et al. Celiac disease Arch Dematol 1984; 120: 994.
and recurrent aphthous stomatitis. Oral Surg Oral Med Oral 42 Sakane T, Takeno M, Suzuki N, et al. Behcets disease. N Engl J
Pathol Oral Radiol Endod 2002; 94: 4748. Med 1999; 341: 128491.
25 Meini A, Pillan MN, Plebani A, et al. High prevalence of 43 International Study Group for Behcets Disease. Criteria
DRW10 and DQW1 antigens in celiac disease associated with for diagnosis of Behcets disease. Lancet 1990; 335: 107880.
recurrent aphthous stomatitis. Am J Gastroenterol 1993; 88: 44 Main DM, Chamberlain MA. Clinical differentiation of oral
972. ulceration in Behcets disease. Br J Rheumatol 1992; 31: 767
26 Scully C, Gorsky M, Lozada-Nur F. The diagnosis and man- 70.
agement of recurrent aphthous stomatitis: a consensus 45 Bang D, Hur W, Lee ES, et al. Prognosis and clinical relevance
approach. J Am Dent Assoc 2003; 134: 2007. of recurrent oral ulceration in Behcets disease. J Dermatol
27 Wray D. Gluten-sensitive recurrent aphthous stomatitis. Dig 1995; 22: 9269.
Dis Sci 1981; 26: 73740. 46 Lehner T. Immunopathogenesis of Behcets disease. Ann Med
28 Wright A, Ryan FP, Willingham SE, et al. Food allergy or Interne (Paris) 1999; 150: 4837.
intolerance in severe recurrent aphthous ulceration of the 47 Lehner T. The role of heat shock protein, microbial and
mouth. Br Med J (Clin Res Edn) 1986; 292: 12378. autoimmune agents in the aetiology of Behcets disease. Int
29 Hunter IP, Ferguson MM, Scully C, et al. Effects of dietary Rev Immunol 1997; 14: 2132.
gluten elimination in patients with recurrent minor aphthous 48 Fortune F. Can you catch Behcets disease? J Labor Clin Med
stomatitis and no detectable gluten enteropathy. Oral Surg 2003; 141: 56.
Oral Med Oral Pathol 1993; 75: 5958. 49 Lehner T, Fortune F, Lavery E, Studd M. Recent advances in T
30 Olson JA, Feinberg I, Silverman S, et al. Serum vitamin B12, cell immunoregulation and the microbial causes of Behcets
folate and iron levels in recurrent aphthous ulceration. Oral disease. In: ODuffy, JD, Kokmen, E, eds. Behcets Disease:
Surg Oral Med Oral Pathol 1982; 54: 51720. Basic and Clinical Aspects. New York: Marcel Dekker, 1991:
31 Porter S, Flint S, Scully C, et al. Recurrent aphthous stomatitis; 46373.
the efficacy of replacement therapy in patients with underly- 50 Ferrick DA, Schrenzel MD, Mulvania T, et al. Differential
ing haematinic deficiencies. Ann Dent 1992; 51: 146. production of interferon-gamma and interlukin-4 in response
32 Muzyka BC, Glick M. Major aphthous ulcers in patients with HIV to Th1- and Th2- stimulating pathogens by gamma delta T
disease. Oral Surg Oral Med Oral Pathol 1994; 77: 11620. cells in vivo. Nature 1995; 373: 2557.
33 MacPhail LA, Greenspan D, Feigal DW, et al. Recurrent aph- 51 Ehrlich GE. Vasculitis in Behcets disease. Int Rev Immunol
thous ulcers in association with HIV infection. Description of 1997; 14: 818.
ulcer types and analysis of T lymphocyte subsets. Oral Surg 52 Yazici H, Barnes CG. Practical treatment recommendations for
Oral Med Oral Pathol 1991; 71: 67883. pharmacotherapy of Behcets syndrome. Drugs 1991; 42:
34 Vanderhoof JA, Rich KC, Stiehm ER, et al. Esophageal ulcers in 796804.
immunodeficiency with elevated levels of IgM and neutrope- 53 Russell AI, Lawson WA, Haskard DO. Potential new thera-
nia. Am J Dis Child 1977; 131: 5512. peutic options in Behcets syndrome. Biodrugs 2001; 5: 2535.
2003 Blackwell Publishing Ltd, Aliment Pharmacol Ther 18, 949962
962 E. A. FIELD & R. B. ALLAN
54 Meador R, Ehrlich G, Von Feldt JM. Behcets disease: 69 Forman L. Two cases of pyodermatatitis vegetans (Hallopeau):
immunopathologic and therapeutic aspects. Current Rheu- an eosinophilic pustular and vegetating dermatitis with con-
matol Rep 2002; 4: 4754. junctival, oral and colonic involvement. Proc R Soc Med
55 Sakane T, Takeno M. Novel approaches to Behcets disease. 1965; 58: 2449.
Expert Opin Invest Drugs 2000; 9: 19932005. 70 Healy CM, Farthing PM, Williams DM, et al. Pyostomatitis
56 Hamuryudan V, Mat C, Saip C, et al. Thalidomide in the vegetans and associated systemic disease: a review and two
treatment of the mucocutaneous lesions of the Behcets syn- case reports. Oral Surg Oral Med Oral Pathol 1994; 78: 323
drome. A randomised double-blind, placebo-controlled trial. 8.
Ann Intern Med 1998; 128: 44350. 71 Margoles JS, Wenger J. Stomal ulceration associated with
57 Kaklamani VG, Kaklamanis PG. Treatment of Behcets pyoderma gangrenosum and ulcerative colitis. Gastroenter-
disease an update. Semin Arthritis Rheum 2001; 5: 299 ology 1961; 41: 5948.
312. 72 Asquith P, Thomson RA, Cooke WT. Oral manifestations of
58 Gardiner-Medwin JM, Smith NJ, Powell RJ. Clinical experience Crohns disease. Gut 1975; 16: 124954.
with thalidomide in the management of severe oral and 73 McLeod RI. Drug-induced aphthous ulcers. Br J Dermatol
genital ulceration in conditions such as Behcets disease: use 2000; 143: 11379.
of neurophysiological studies to detect thalidomide neuropa- 74 Dellinger TM, Livingston HM. Aspirin burn of the oral cavity.
thy. Ann Rheum Dis 1994; 53: 82832. Ann Pharmacotherapy 1998; 32: 1107.
59 Adler YD, Mansmann U, Zouboulis CC. Mycophenolate mofetil 75 Royal Pharmaceutical Society of. Great Britain and the British
is ineffective in the treatment of mucocutaneous Adamanti- Medical Association. British National Formulary. 2003; 45:
adesBehcets disease. Dermatology 2001; 203: 3224. 60, 492.
60 Miyachi Y, Tangiguchi S, Ozaki M, et al. Colchicine in the 76 Wakham MD, McNeal Dr Burtner AP. Pouching of medica-
treatment of the cutaneous manifestations of Behcets disease. tions in the mouth: a case report. Spec Care Dentist 1990;
Br J Dermatol 1981; 104: 679. 10: 913.
61 Sfikakis PP. Behcets disease: a new target for anti-tumour 77 Cohen DM, Bhattacharyya I, Lydiatt WM. Recalcitrant oral
necrosis factor treatment. Ann Rheum Dis 2002; 61(Suppl. ulcers caused by calcium channel blockers. diagnosis and
2): ii513. treatment considerations. J Am Dent Assoc 1999; 130: 16118.
62 Robertson LP, Hickling P. Treatment of recalcitrant orogenital 78 Healy CM, Thornhill MH. An association between recurrent
ulceration of Behcets syndrome with infliximab. Rheumatol- oro-genital ulceration and non-steroidal anti-inflammatory
ogy (Oxford) 2001; 40: 4734. drugs. J Oral Pathol Med 1995; 1: 468.
63 Wiesenfeld D, Ferguson MM, Mitchell DN, et al. Oro-facial 79 Shotts RH, Scully C, Avery CM, et al. Nicorandil-induced
granulomatosis a clinical and pathological analysis. Q J Med severe oral ulceration: a newly recognised drug reaction.
1985; 54: 10113. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999; 87:
64 Sweatman MC, Tasker R, Warner JO, et al. Oro-facial gra- 7067.
nulomatosis. Response to elemental diet and provocation by 80 Scully C, Azul AM, Crighton A, et al. Nicorandil can induce
food additives. Clin Allergy 1986; 16: 3318. severe oral ulceration. Oral Surg Oral Med Oral Pathol Oral
65 Haworth RJ, MacFadyen EE, Ferguson MM. Food intolerance Radiol Endod 2001; 91: 18993.
in patients with oro-facial granulomatosis. Hum Nutr Appl 81 Desruelles F, Bahadoran P, Lacour JP, et al. Giant oral aph-
Nutr 1986; 40: 44756. thous ulcers induced by nicorandil. Br J Dermatol 1998; 138:
66 Gibson J, Wray D, Bagg J. Oral staphylococcal mucositis. 7123.
A new clinical entity in orofacial granulomatosis and Crohns 82 Lam PP. Severe stomatitis caused by penicillamine. Br Dent J
disease. Oral Surg, Oral Med, Oral Path Oral Pathol Oral 1980; 149: 1801.
Radiol Endod 2000; 89: 1716. 83 Bauer J, Fartasch M, Schuler G, et al. Ulcerative stomatitis as
67 Field EA. Oral Lesions in IBD. Inflammatory Bowel Disease clinical clue to inadvertent methotrexate overdose. Hautarzt
Monitor 2001; 2: 6672. 1999; 50: 6703.
68 Thornhill MH, Zakrzewska JM, Gilkes JJ. Pyostomatitis vege- 84 Singh N, Scully C, Joyston-Bechal S. Oral complications of
tans. report of three cases and review of the literature. J Oral cancer therapies: prevention and management. Clin Oncol
Pathol Med 1992; 21: 12833. 1996; 8: 1524.
2003 Blackwell Publishing Ltd, Aliment Pharmacol Ther 18, 949962
You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Low-sodium soup and protein shake optionsDocument5 pagesLow-sodium soup and protein shake optionsMara DiasNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- GRAINS AND CEREALS: A GUIDE TO TYPES AND BENEFITSDocument29 pagesGRAINS AND CEREALS: A GUIDE TO TYPES AND BENEFITSJoan Eda De Vera100% (1)
- Ayurveda Q&A - Detoxification Therapy Cures Fungal Infection - Sify HealthDocument12 pagesAyurveda Q&A - Detoxification Therapy Cures Fungal Infection - Sify Healthsanti_1976No ratings yet
- f2021 SyllabusDocument6 pagesf2021 SyllabusRaging PotatoNo ratings yet
- High Pressure Processing Presentation by Bhawani KurreDocument19 pagesHigh Pressure Processing Presentation by Bhawani KurreMayur KadamNo ratings yet
- Nutrition NotesDocument5 pagesNutrition Notesdrng48No ratings yet
- Drugs PregnancyDocument9 pagesDrugs PregnancyPamelaS9No ratings yet
- F4cd8a06d3a63e4463e31f34 PDFDocument3 pagesF4cd8a06d3a63e4463e31f34 PDFRinaldi InalNo ratings yet
- Length-For-Age BOYS: Birth To 6 Months (Z-Scores)Document1 pageLength-For-Age BOYS: Birth To 6 Months (Z-Scores)Malisa LukmanNo ratings yet
- Kehamilan Dan Periodontal PDFDocument7 pagesKehamilan Dan Periodontal PDFBellia MarsyaNo ratings yet
- Abscess Remedy PasteDocument1 pageAbscess Remedy PasteAyu NurlailaNo ratings yet
- Jurnal OrtognatikDocument7 pagesJurnal OrtognatikRinaldi InalNo ratings yet
- Elsa 19.4Document6 pagesElsa 19.4salsabilakrnNo ratings yet
- Instruction For Use Zinc Oxide Eugenol-Based Root Canal Sealer "Eugetin" IndicationsDocument2 pagesInstruction For Use Zinc Oxide Eugenol-Based Root Canal Sealer "Eugetin" IndicationsSalma MentariNo ratings yet
- Acute Herpetic Gingivostomatitis in Adults: A Review of 13 Cases, Including Diagnosis and ManagementDocument5 pagesAcute Herpetic Gingivostomatitis in Adults: A Review of 13 Cases, Including Diagnosis and ManagementAfaf MahmoudNo ratings yet
- Heliosit OrthodonticDocument20 pagesHeliosit OrthodonticAndhika Galih PrasetyoNo ratings yet
- Bahan Jurnal Dokter Ida 2Document5 pagesBahan Jurnal Dokter Ida 2Rinaldi InalNo ratings yet
- Dentists and Demographics: American Dental Education AssociationDocument4 pagesDentists and Demographics: American Dental Education AssociationGaleri Kreasi SepatukuNo ratings yet
- Comprehensive Periodontal Exam GuideDocument40 pagesComprehensive Periodontal Exam GuideKavin SandhuNo ratings yet
- Dentists and Demographics: American Dental Education AssociationDocument4 pagesDentists and Demographics: American Dental Education AssociationGaleri Kreasi SepatukuNo ratings yet
- SAR Dan TraumaDocument2 pagesSAR Dan TraumaRinaldi InalNo ratings yet
- Bahan OM Bab 4 PDFDocument3 pagesBahan OM Bab 4 PDFRinaldi InalNo ratings yet
- Drug Allergy: National Clinical Guideline CentreDocument167 pagesDrug Allergy: National Clinical Guideline CentreRinaldi InalNo ratings yet
- Cleaning and Shaping 2006 FinalDocument60 pagesCleaning and Shaping 2006 FinalKapil JhajhariaNo ratings yet
- Adhesivedentistry GlassIonomers PDFDocument10 pagesAdhesivedentistry GlassIonomers PDFRinaldi InalNo ratings yet
- GicDocument5 pagesGicmrnitin82No ratings yet
- Glass IonomerDocument6 pagesGlass IonomerRinaldi InalNo ratings yet
- Allergy Diagnostic TestingDocument149 pagesAllergy Diagnostic TestingIoana-NicoletaNicodimNo ratings yet
- 899 - GeneralConsiderations On Drug HyperDocument7 pages899 - GeneralConsiderations On Drug HyperRinaldi InalNo ratings yet
- GIC FujiDocument4 pagesGIC FujiRinaldi InalNo ratings yet
- Tugas Inggris IchaDocument1 pageTugas Inggris IchaRinaldi InalNo ratings yet
- 2010 Drug AllergyDocument78 pages2010 Drug AllergyEve Methaw100% (1)
- Guidelines For Testing SkinDocument8 pagesGuidelines For Testing SkinRinaldi InalNo ratings yet
- Drugs AdministrationDocument33 pagesDrugs AdministrationRinaldi InalNo ratings yet
- Commonly Prescribed Medications in Pediatric Dentistry: Steven Schwartz, DDSDocument25 pagesCommonly Prescribed Medications in Pediatric Dentistry: Steven Schwartz, DDSSumit BediNo ratings yet
- How a Village Overcame MalnutritionDocument22 pagesHow a Village Overcame Malnutritionmarch20poojaNo ratings yet
- Food Fortification ProgramDocument5 pagesFood Fortification ProgramChar PereaNo ratings yet
- Digestibility Determination in Fish Using Chromic Oxide Marking and Analysis of Contents From Different Segments of The Gastrointestinal TractDocument8 pagesDigestibility Determination in Fish Using Chromic Oxide Marking and Analysis of Contents From Different Segments of The Gastrointestinal TractRafael Hamakawa ViannaNo ratings yet
- Heart Failure Clinical Pathway GuideDocument7 pagesHeart Failure Clinical Pathway GuidedjizhieeNo ratings yet
- Dietabajaencarbohidratos Moreno Capponi 2020Document11 pagesDietabajaencarbohidratos Moreno Capponi 2020PerlaNo ratings yet
- Feasibility Study On Production of RasaposhaDocument42 pagesFeasibility Study On Production of Rasaposhaesubalew sintieNo ratings yet
- Bio 203Document10 pagesBio 203madison dworskyNo ratings yet
- KCL Drug For RespectDocument4 pagesKCL Drug For RespectJamal LiaqatNo ratings yet
- An Introduction To Vitamins Minerals and WaterDocument2 pagesAn Introduction To Vitamins Minerals and WaterAnonymous XIwe3KKNo ratings yet
- CP 83 030Document215 pagesCP 83 030alinapascuNo ratings yet
- Resume For AsanteDocument2 pagesResume For Asanteapi-239305061No ratings yet
- Adolescent Development ArticleDocument8 pagesAdolescent Development Articleapi-308979239No ratings yet
- 5 2474 20110126165113 00001Document10 pages5 2474 20110126165113 00001John Mark Rigor ComelioNo ratings yet
- ISA Brown Guide Nov. 3 2010Document42 pagesISA Brown Guide Nov. 3 2010Cristi Chihaia100% (5)
- HypocalcemiaDocument2 pagesHypocalcemiaRachel Frances SorillaNo ratings yet
- Oferta SC AMNIOCEN DISTRIBUTIE SRL 25.10.2019Document2 pagesOferta SC AMNIOCEN DISTRIBUTIE SRL 25.10.2019Nume PrenumeNo ratings yet
- Public Health Nutrition-I: National Agencies Engaged in Food and Nutrition Activities - Icmr - NinDocument17 pagesPublic Health Nutrition-I: National Agencies Engaged in Food and Nutrition Activities - Icmr - NinBarbie mendroliaNo ratings yet
- Miriam's Must Haves: Dewey 600Document8 pagesMiriam's Must Haves: Dewey 600PRHLibraryNo ratings yet
- A 47 YearDocument12 pagesA 47 Yearwira rila zulma67% (3)
- Glositis PDFDocument1 pageGlositis PDFNenny HariyantoNo ratings yet
- Nutrition Guide for Managing Metabolic SyndromeDocument59 pagesNutrition Guide for Managing Metabolic SyndromeRadya AgnaNo ratings yet
- Chemical Composition and Nutritional Value of Emmer Wheat (Triticum Dicoccon Schrank) : A ReviewDocument18 pagesChemical Composition and Nutritional Value of Emmer Wheat (Triticum Dicoccon Schrank) : A Reviewthor ragnarokNo ratings yet
- Anemia FerropenicaDocument10 pagesAnemia FerropenicaDiany ChivitaNo ratings yet
- Womens Health India March 2014Document124 pagesWomens Health India March 2014NishimaNo ratings yet