You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Final Year Project Proposal in Food Science and TechnologyDocument11 pagesFinal Year Project Proposal in Food Science and TechnologyDEBORAH OSOSANYANo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Marketing ManagementDocument228 pagesMarketing Managementarpit gargNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Outline 2018: Cultivating Professionals With Knowledge and Humanity, Thereby Contributing To People S Well-BeingDocument34 pagesOutline 2018: Cultivating Professionals With Knowledge and Humanity, Thereby Contributing To People S Well-BeingDd KNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- MCQ Chapter 1Document9 pagesMCQ Chapter 1K57 TRAN THI MINH NGOCNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Chap 2 Tanner - The Sales Function & Multi Sales Channels 280516Document17 pagesChap 2 Tanner - The Sales Function & Multi Sales Channels 280516Shahzain RafiqNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- RA 9072 (National Cave Act)Document4 pagesRA 9072 (National Cave Act)Lorelain ImperialNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Veronica Guerin Interview With Anne FelloniDocument2 pagesVeronica Guerin Interview With Anne FelloniDeclan Max BrohanNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Online Learning Can Replace Classroom TeachingsDocument7 pagesOnline Learning Can Replace Classroom TeachingsSonam TobgayNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
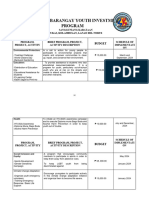
- Annual Barangay Youth Investment ProgramDocument4 pagesAnnual Barangay Youth Investment ProgramBarangay MukasNo ratings yet
- People V CarlosDocument1 pagePeople V CarlosBenBulacNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Isa 75.03 1992 PDFDocument14 pagesIsa 75.03 1992 PDFQuang Duan NguyenNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Problem Set 2Document2 pagesProblem Set 2nskabra0% (1)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Bow IwrbsDocument4 pagesBow IwrbsRhenn Bagtas SongcoNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- History and Theory of Human Rights PDFDocument7 pagesHistory and Theory of Human Rights PDFCustom Writing ServicesNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Continuous Improvement Requires A Quality CultureDocument12 pagesContinuous Improvement Requires A Quality Culturespitraberg100% (19)
- Type Certificate Data Sheet: No. EASA.R.100Document9 pagesType Certificate Data Sheet: No. EASA.R.100SauliusNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- TEST Inter. U.1 Name: - : Grammar 1 Underline The Correct FormDocument4 pagesTEST Inter. U.1 Name: - : Grammar 1 Underline The Correct FormKrisztofer Török100% (1)
- Price Controls and Quotas: Meddling With MarketsDocument53 pagesPrice Controls and Quotas: Meddling With MarketsMarie-Anne RabetafikaNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Marudur,+6 +nikaDocument12 pagesMarudur,+6 +nikaResandi MuhamadNo ratings yet
- Strategy Output Activity (Ppa) : Activities (Ppas) For The Social Sector Activities (Ppas) For The Education Sub-SectorDocument3 pagesStrategy Output Activity (Ppa) : Activities (Ppas) For The Social Sector Activities (Ppas) For The Education Sub-Sectorstella marizNo ratings yet
- Micro PPT FinalDocument39 pagesMicro PPT FinalRyan Christopher PascualNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Toms River Fair Share Housing AgreementDocument120 pagesToms River Fair Share Housing AgreementRise Up Ocean CountyNo ratings yet
- Course SyllabusDocument9 pagesCourse SyllabusJae MadridNo ratings yet
- Criticism of DAT SutherlandDocument2 pagesCriticism of DAT SutherlandBabarNo ratings yet
- Philippine Stock Exchange: Head, Disclosure DepartmentDocument58 pagesPhilippine Stock Exchange: Head, Disclosure DepartmentAnonymous 01pQbZUMMNo ratings yet
- The Consequences of Using Incorrect TerminologyDocument6 pagesThe Consequences of Using Incorrect TerminologyPastor DavidNo ratings yet
- Case Study No. 8-Managing Floods in Metro ManilaDocument22 pagesCase Study No. 8-Managing Floods in Metro ManilapicefeatiNo ratings yet
- Implementing OSPF RoutingDocument20 pagesImplementing OSPF RoutingHuỳnh Tấn LợiNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- EPS For OPAPRU Executives - Ao24jan2024Document3 pagesEPS For OPAPRU Executives - Ao24jan2024rinafenellere.opapruNo ratings yet
- Patrick Svitek - Resume 2012Document1 pagePatrick Svitek - Resume 2012Patrick SvitekNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)