You might also like
- Immediate Post Anesthetic RecoveryDocument12 pagesImmediate Post Anesthetic Recoverysubvig100% (2)
- CCCDocument487 pagesCCCSlaviša KovačevićNo ratings yet
- Preoperative Assessment and Premedication - PACUDocument60 pagesPreoperative Assessment and Premedication - PACUTraceNo ratings yet
- ESUR Guidelines On Contrast MediaDocument10 pagesESUR Guidelines On Contrast MediatsimitselisNo ratings yet
- Chronic Pain SAQ'sDocument52 pagesChronic Pain SAQ'sNaser AhmedNo ratings yet
- Graphic Anaesthesia, second edition: Essential diagrams, equations and tables for anaesthesiaFrom EverandGraphic Anaesthesia, second edition: Essential diagrams, equations and tables for anaesthesiaNo ratings yet
- Ultrasound-Guided Block of TheDocument6 pagesUltrasound-Guided Block of Theandrew herringNo ratings yet
- Gautam Das Clinical ExaminationDocument233 pagesGautam Das Clinical ExaminationHenry SugihartoNo ratings yet
- Minimally Invasive Surgery for Chronic Pain Management: An Evidence-Based ApproachFrom EverandMinimally Invasive Surgery for Chronic Pain Management: An Evidence-Based ApproachGiorgio PietramaggioriNo ratings yet
- Regional 53Document53 pagesRegional 53RaMy “MhMd” ElaRabyNo ratings yet
- Bone Marrow Aspirate Concentrate and Expanded Stem Cell Applications in OrthopaedicsFrom EverandBone Marrow Aspirate Concentrate and Expanded Stem Cell Applications in OrthopaedicsNo ratings yet
- Who Analgesic LadderDocument55 pagesWho Analgesic LadderSyifa Nurul Asma'No ratings yet
- Peng 2015 PDFDocument1,002 pagesPeng 2015 PDFLore BarreraNo ratings yet
- 2022 Stoelting's AnesthesiaDocument723 pages2022 Stoelting's AnesthesiaPedro Maçada AndradeNo ratings yet
- Advanced Endovascular Therapy of Aortic DiseaseFrom EverandAdvanced Endovascular Therapy of Aortic DiseaseAlan B. LumsdenNo ratings yet
- Copy-Question PapersDocument87 pagesCopy-Question Paperspooja patilNo ratings yet
- Algology ModuleDocument2 pagesAlgology ModulerosanowardNo ratings yet
- Cardiology Ultrasound EmergencyDocument92 pagesCardiology Ultrasound Emergencybeeluvit81444No ratings yet
- Blood Pressure Regulation SummaryDocument42 pagesBlood Pressure Regulation SummaryLouis JinNo ratings yet
- Complication of Spina AnesthesiaDocument8 pagesComplication of Spina AnesthesiaSandroLaoNo ratings yet
- ORIF Ankle Surgery RecoveryDocument2 pagesORIF Ankle Surgery RecoverypatzieNo ratings yet
- Pediatric Anesthesiology Review: Clinical Cases for Self-AssessmentFrom EverandPediatric Anesthesiology Review: Clinical Cases for Self-AssessmentNo ratings yet
- Overview of Complications Occurring in The Post-Anesthesia Care UnitDocument14 pagesOverview of Complications Occurring in The Post-Anesthesia Care UnitShahabuddin ShaikhNo ratings yet
- OSA and Periop Complications 2012Document9 pagesOSA and Periop Complications 2012cjbae22No ratings yet
- Regional Nerve Blocks And Infiltration Therapy: Textbook and Color AtlasFrom EverandRegional Nerve Blocks And Infiltration Therapy: Textbook and Color AtlasDanilo JankovicNo ratings yet
- Practice Guidelines For Juniors 01 June 2016Document3 pagesPractice Guidelines For Juniors 01 June 2016ElaineNo ratings yet
- Clinical Indications For MSK UltrasoundDocument10 pagesClinical Indications For MSK Ultrasoundapi-263772125No ratings yet
- Recommended Reading List For EDAIC 2019Document5 pagesRecommended Reading List For EDAIC 2019Bebo EsmatNo ratings yet
- Testicular TorsionDocument9 pagesTesticular TorsionSyedKashifAliNo ratings yet
- Updates Clinical: International Association For The Study of PainDocument6 pagesUpdates Clinical: International Association For The Study of PainSuaeni Kurnia WirdaNo ratings yet
- Oxford Handbook of Clinical Medicine 11eDocument93 pagesOxford Handbook of Clinical Medicine 11ethesagordeyNo ratings yet
- Manejo de Las Crisis en Anestesia - Gaba 2 Ed PDFDocument424 pagesManejo de Las Crisis en Anestesia - Gaba 2 Ed PDFdianisssuxNo ratings yet
- The stellate ganglion is located anterior to the transverse processes of C7 and T1 vertebraeDocument287 pagesThe stellate ganglion is located anterior to the transverse processes of C7 and T1 vertebraeSAJID ALINo ratings yet
- EVAR Anes 2016Document10 pagesEVAR Anes 2016Joey PunjasaNo ratings yet
- Pain Relief in Palliative Care, A Focus On Interventional Pain Management PDFDocument11 pagesPain Relief in Palliative Care, A Focus On Interventional Pain Management PDFShinichi Ferry RoferdiNo ratings yet
- Ultrasound Guided Interventional Procedures In.4Document13 pagesUltrasound Guided Interventional Procedures In.4andrew herringNo ratings yet
- Women's Imaging: MRI with Multimodality CorrelationFrom EverandWomen's Imaging: MRI with Multimodality CorrelationMichele A. BrownRating: 5 out of 5 stars5/5 (1)
- Ultrasound-Guided Intervention Around The Hip Joint: Emma L. Rowbotham Andrew J. GraingerDocument6 pagesUltrasound-Guided Intervention Around The Hip Joint: Emma L. Rowbotham Andrew J. Graingerandrew herringNo ratings yet
- Clarks Essential Guide To Clinical UltrasoundDocument77 pagesClarks Essential Guide To Clinical Ultrasoundrobertlinon0% (1)
- MR Okor SAC Neurosurgery CVDocument8 pagesMR Okor SAC Neurosurgery CVdrokor8747No ratings yet
- Exam ANS Report Final2022 1 PRVDocument18 pagesExam ANS Report Final2022 1 PRVtestingNo ratings yet
- Usg 20088Document18 pagesUsg 20088iridaNo ratings yet
- Hill - Workshop - Intro To MSK US Shoulder WS 2014-1Document32 pagesHill - Workshop - Intro To MSK US Shoulder WS 2014-1Raihan LuthfiNo ratings yet
- Essential anesthesia room setup checklistDocument31 pagesEssential anesthesia room setup checklistnbrassarNo ratings yet
- Cervical Spine Trauma Imaging GuideDocument25 pagesCervical Spine Trauma Imaging GuideComagaNo ratings yet
- Contrast Agents, Cath Lab & Anaphylatic Shock-ParamedDocument29 pagesContrast Agents, Cath Lab & Anaphylatic Shock-ParamedManikanta GupthaNo ratings yet
- AWARENESS UNDER ANESTHESIA: DEFINITION, TYPES, RISK FACTORS & PREVENTIONDocument27 pagesAWARENESS UNDER ANESTHESIA: DEFINITION, TYPES, RISK FACTORS & PREVENTIONagatakassaNo ratings yet
- A Case-Based Approach to Interventional Pulmonology: A Focus on Asian PerspectivesFrom EverandA Case-Based Approach to Interventional Pulmonology: A Focus on Asian PerspectivesJamalul Azizi Abdul RahamanNo ratings yet
- 1stprize CR Auditpostercomp C Reid 2015Document1 page1stprize CR Auditpostercomp C Reid 2015webber_denzNo ratings yet
- Geriatric NeuroanesthesiDocument333 pagesGeriatric NeuroanesthesiAdi Wira HadiNo ratings yet
- Year One of Practice Transition: The Necessary Guide to SuccessFrom EverandYear One of Practice Transition: The Necessary Guide to SuccessJason E. PopeNo ratings yet
- ERAS in PaediatricsDocument29 pagesERAS in Paediatricscasco100% (1)
- Hadzic's Peripheral Nerve Blocks and Anatomy For Ultrasound Guided Regional Anesthesia (New York School of Regional Anesthesia) PDF DownloadDocument3 pagesHadzic's Peripheral Nerve Blocks and Anatomy For Ultrasound Guided Regional Anesthesia (New York School of Regional Anesthesia) PDF Downloadhellena buks33% (3)
- Sachin Khanduri - Textbook of Radiology For X-Ray, CT, MRI, BSC, BRIT and MSC Technicians 2EDocument1 pageSachin Khanduri - Textbook of Radiology For X-Ray, CT, MRI, BSC, BRIT and MSC Technicians 2EImrose MahineNo ratings yet
- Anesthesia For Major Urologic Surgery: James O.B. Cockcroft,, Colin B. Berry,, John S. Mcgrath,, Mark O. DaughertyDocument8 pagesAnesthesia For Major Urologic Surgery: James O.B. Cockcroft,, Colin B. Berry,, John S. Mcgrath,, Mark O. DaughertyJEFFERSON MUÑOZNo ratings yet
- Author Section Editor Deputy Editor Contributor DisclosuresDocument10 pagesAuthor Section Editor Deputy Editor Contributor DisclosuresannisNo ratings yet
- Protocol 4 SlicesDocument143 pagesProtocol 4 SlicessaeedNo ratings yet
- 455657Document2 pages455657Madyline VictoryaNo ratings yet
- SOFA Score Describes Organ DysfunctionDocument4 pagesSOFA Score Describes Organ DysfunctionMadyline VictoryaNo ratings yet
- CohotDocument14 pagesCohotMadyline VictoryaNo ratings yet
- AP MR GlossaryDocument5 pagesAP MR GlossaryReynaldi HadiwijayaNo ratings yet
- NelsonDocument1 pageNelsonMadyline VictoryaNo ratings yet
- Paincontrol PDFDocument52 pagesPaincontrol PDFMadyline VictoryaNo ratings yet
- KKR - 8 Mei 2014Document2 pagesKKR - 8 Mei 2014Madyline VictoryaNo ratings yet
- Jadwal Piket Perawat Rawat IanapDocument18 pagesJadwal Piket Perawat Rawat IanapMadyline Victorya100% (1)
- Age Ageing-2013 - I1-I57Document57 pagesAge Ageing-2013 - I1-I57Madyline VictoryaNo ratings yet
- Secrets to Long Life Revealed in Blue ZonesDocument10 pagesSecrets to Long Life Revealed in Blue ZonesMadyline VictoryaNo ratings yet
- Adosex 1Document52 pagesAdosex 1Madyline VictoryaNo ratings yet
- Journal ReadingDocument23 pagesJournal ReadingMadyline VictoryaNo ratings yet
- Gizi SeimbangDocument54 pagesGizi SeimbangMarliana PohanNo ratings yet
- Standards of Good Practice For Spinal Interventional ProceduresDocument20 pagesStandards of Good Practice For Spinal Interventional ProceduresMadyline VictoryaNo ratings yet
- SpiritualityDocument82 pagesSpiritualityMadyline VictoryaNo ratings yet
- 2006 8215Document86 pages2006 8215Madyline VictoryaNo ratings yet
- Ectopic PregnancyDocument16 pagesEctopic PregnancyMadyline VictoryaNo ratings yet
- Referat RadiologiDocument6 pagesReferat RadiologiMadyline VictoryaNo ratings yet
- EmpyemaDocument27 pagesEmpyemaMadyline VictoryaNo ratings yet
- Obstetric Abdominal ExaminationDocument32 pagesObstetric Abdominal ExaminationMadyline VictoryaNo ratings yet
- Anestesi and FESSDocument6 pagesAnestesi and FESSMadyline VictoryaNo ratings yet
- Basic Life SupportDocument12 pagesBasic Life SupportMadyline VictoryaNo ratings yet
- Socialism CapitalismDocument268 pagesSocialism CapitalismRobert PattonNo ratings yet
- Secrets to Long Life Revealed in Blue ZonesDocument10 pagesSecrets to Long Life Revealed in Blue ZonesMadyline VictoryaNo ratings yet
- Hasil Kontrol LisaDocument2 pagesHasil Kontrol LisaMadyline VictoryaNo ratings yet
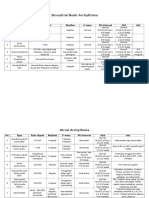
- Sinoatrial Node Arrhythmia: No Type Rate (BPM) Rhythm P Wave PR Interval ORS KetDocument3 pagesSinoatrial Node Arrhythmia: No Type Rate (BPM) Rhythm P Wave PR Interval ORS KetMadyline VictoryaNo ratings yet
- Cardiology Research EvaluationDocument6 pagesCardiology Research EvaluationMadyline VictoryaNo ratings yet
- Pub Prof EpiduralAnalgesia2010Document14 pagesPub Prof EpiduralAnalgesia2010Madyline VictoryaNo ratings yet
- Pain Assess Breakthrough Pain HagenDocument8 pagesPain Assess Breakthrough Pain HagenMadyline VictoryaNo ratings yet
- Organizational Behavior: Stephen P. RobbinsDocument35 pagesOrganizational Behavior: Stephen P. RobbinsPariManiyarNo ratings yet
- Grade 12 Class Achievements for 2018-2019 School YearDocument3 pagesGrade 12 Class Achievements for 2018-2019 School YearRhaedenNarababYalanibNo ratings yet
- Artificial Intelligence Applications in Civil EngineeringDocument31 pagesArtificial Intelligence Applications in Civil Engineeringpuppyarav2726No ratings yet
- EMZ 7e's Lesson PlanDocument5 pagesEMZ 7e's Lesson PlanEmily Tatunay EspejoNo ratings yet
- Houran - Do Online Matchmaking Tests WorkDocument21 pagesHouran - Do Online Matchmaking Tests Workyasirzaidi1No ratings yet
- Reinabelle Reyes (Batch 2001) Reinabelle Reyes (Batch 2001) : The Life of Rodel Lasco, PHD (Batch 1977)Document2 pagesReinabelle Reyes (Batch 2001) Reinabelle Reyes (Batch 2001) : The Life of Rodel Lasco, PHD (Batch 1977)Rivera MaeNo ratings yet
- (International Library of Technical and Vocational Education and Training) Felix Rauner, Rupert Maclean (Auth.), Felix Rauner, Rupert Maclean (Eds.) - Handbook of Technical and Vocational Educatio PDFDocument1,090 pages(International Library of Technical and Vocational Education and Training) Felix Rauner, Rupert Maclean (Auth.), Felix Rauner, Rupert Maclean (Eds.) - Handbook of Technical and Vocational Educatio PDFAulia YuanisahNo ratings yet
- Barking Abbey Basketball AcademyDocument11 pagesBarking Abbey Basketball AcademyAbbeyBasketballNo ratings yet
- The Effect of Parenting Style of A Single Parent To Manage Their GenDocument11 pagesThe Effect of Parenting Style of A Single Parent To Manage Their GenFranchel Kaye EstayoNo ratings yet
- Primera Lengua Extranjera II - Inglés Examen ResueltoDocument4 pagesPrimera Lengua Extranjera II - Inglés Examen ResueltoAlbaNo ratings yet
- DiversityDocument3 pagesDiversityapi-464306934No ratings yet
- Guidance for internal audit standards implementationDocument8 pagesGuidance for internal audit standards implementationkaranziaNo ratings yet
- Introduction To Paralegalism Instructors ManualDocument12 pagesIntroduction To Paralegalism Instructors Manualonerussian11% (9)
- REVISED - Teamwork Reflection - UNIT 10 PMAL - AAKASHDocument5 pagesREVISED - Teamwork Reflection - UNIT 10 PMAL - AAKASHjackfcuk1No ratings yet
- FEU Intro to Architectural Visual 3 and One Point PerspectiveDocument2 pagesFEU Intro to Architectural Visual 3 and One Point Perspectiveangelle cariagaNo ratings yet
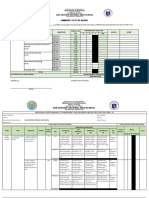
- IPCRF Form TeachersDocument9 pagesIPCRF Form TeachersrafaelaNo ratings yet
- 974Document34 pages974B. MerkurNo ratings yet
- Brahmavidya Breathing SummeryDocument13 pagesBrahmavidya Breathing Summerysudhir vaidya100% (1)
- Educational Services Post Secondary Education Award Ma000075 Pay GuideDocument34 pagesEducational Services Post Secondary Education Award Ma000075 Pay Guiderabi1973No ratings yet
- Talavera South Central School: Alternative Work Arrangement Date and Actual Time Logs Actual AccomplishmentsDocument2 pagesTalavera South Central School: Alternative Work Arrangement Date and Actual Time Logs Actual AccomplishmentsErwin de VillaNo ratings yet
- Lesson 2 - Nature of ResearchDocument11 pagesLesson 2 - Nature of ResearchRuben Rosendal De Asis100% (1)
- Lesson 16 - Designing The Training CurriculumDocument80 pagesLesson 16 - Designing The Training CurriculumCharlton Benedict BernabeNo ratings yet
- TLE Beauty Care (Nail Care) Services: Department of Education - Republic of The PhilippinesDocument38 pagesTLE Beauty Care (Nail Care) Services: Department of Education - Republic of The PhilippinesREYNOLD MILLONDAGA100% (2)
- Cpts 440 / 540 Artificial IntelligenceDocument65 pagesCpts 440 / 540 Artificial IntelligenceDuc Minh LeNo ratings yet
- Vanessa JoyDocument23 pagesVanessa JoyAstigBermudezNo ratings yet
- 18TH AmendmenntDocument36 pages18TH AmendmenntMadiha AbbasNo ratings yet
- Resume - CarlyDocument1 pageResume - Carlyapi-317491156No ratings yet
- Problems Encountered by Teachers in The Teaching-Learning Process: A Basis of An Action PlanDocument20 pagesProblems Encountered by Teachers in The Teaching-Learning Process: A Basis of An Action PlanERIKA O. FADEROGAONo ratings yet
- Affirmative ActionDocument23 pagesAffirmative ActionUtkarsh Mani TripathiNo ratings yet
- Предметно-интегрированное обучение (Clil: Content And Language Integrated Learning) английскому языку на основе применения дистанционных образовательных технологийDocument45 pagesПредметно-интегрированное обучение (Clil: Content And Language Integrated Learning) английскому языку на основе применения дистанционных образовательных технологийНазерке ЧабденоваNo ratings yet