You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- BARU 3 Ptsa 150923Document117 pagesBARU 3 Ptsa 150923Joyoboyo PrimaNo ratings yet
- First Aid Pharmacology AntimicrobialsDocument23 pagesFirst Aid Pharmacology AntimicrobialsLaura Lopez RocaNo ratings yet
- About TulsiDocument3 pagesAbout TulsiNidhi Upadhyay100% (1)
- Dermatology For The Small Animal Practitioner (Made Easy Series)Document163 pagesDermatology For The Small Animal Practitioner (Made Easy Series)Nela Frade0% (1)
- MCP AbxDocument34 pagesMCP AbxShynne RPhNo ratings yet
- Write A Comment... : Cheerful NihilismDocument1 pageWrite A Comment... : Cheerful NihilismKatie bNo ratings yet
- Mycobacterium Abscessus: A New Antibiotic NightmareDocument9 pagesMycobacterium Abscessus: A New Antibiotic NightmareHootNo ratings yet
- Principles of Antimicrobial TherapyDocument39 pagesPrinciples of Antimicrobial TherapyAsthree Nur AzizahNo ratings yet
- Soil Antibiotic ProducerDocument3 pagesSoil Antibiotic ProducerAshen Nirodya0% (1)
- Antibacterial activities of the methanol extracts of Albizia adianthifolia, Alchornea laxiflora, Laportea ovalifolia and three other Cameroonian plants against multi-drug resistant Gram-negative bacteriaDocument6 pagesAntibacterial activities of the methanol extracts of Albizia adianthifolia, Alchornea laxiflora, Laportea ovalifolia and three other Cameroonian plants against multi-drug resistant Gram-negative bacteriaArieNo ratings yet
- Prevent Antimicrobial ResistanceDocument6 pagesPrevent Antimicrobial ResistanceThefatRatNo ratings yet
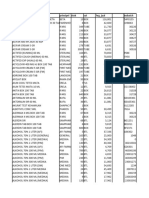
- Inventory Parts Listing with Item Numbers and DescriptionsDocument8 pagesInventory Parts Listing with Item Numbers and DescriptionsNurma Annisa FitriaNo ratings yet
- MC Great Lakes SlidesDocument26 pagesMC Great Lakes Slidesapi-666654042No ratings yet
- Rational Use of AntibioticsDocument85 pagesRational Use of AntibioticsAHMAD MAHIR BIN CHE RAHMATNo ratings yet
- Microorganisms Friend and FoeDocument27 pagesMicroorganisms Friend and Foedotcomddn100% (1)
- Evaluation of Antibacterial & Antioxidant Activities of The Leaf Essential Oil & Leaf Extracts of Citrus AurantifoliaDocument9 pagesEvaluation of Antibacterial & Antioxidant Activities of The Leaf Essential Oil & Leaf Extracts of Citrus AurantifoliaFirman TirmaNo ratings yet
- Medicinal Chemistry GuideDocument23 pagesMedicinal Chemistry Guidemurugs92No ratings yet
- Antimicrobial ChemotherapyDocument160 pagesAntimicrobial Chemotherapyokumu atanas0% (1)
- Clasificator Medicamente 30.11.2016Document1,038 pagesClasificator Medicamente 30.11.2016Cătălina GîlcaNo ratings yet
- Bovine Mastitis SVDocument62 pagesBovine Mastitis SVSatyavrat SinghNo ratings yet
- Form Stock ObatDocument7 pagesForm Stock ObatSyarifahUniqueNo ratings yet
- Aae Endodonticglossary2016Document50 pagesAae Endodonticglossary2016h20pologtNo ratings yet
- RMO Handbook AussieDocument48 pagesRMO Handbook Aussienvrtm43No ratings yet
- Sinus Treatment7 05Document23 pagesSinus Treatment7 05arjuna45No ratings yet
- DR. ARIFIN - CAP (New PDPI Guideline)Document36 pagesDR. ARIFIN - CAP (New PDPI Guideline)Inggriht Senny BondangNo ratings yet
- Antimicrobial Textiles Mechanisms EffectsDocument7 pagesAntimicrobial Textiles Mechanisms Effectsjohn_dominic_4No ratings yet
- Fertizone Product Catalog-14.03.22Document49 pagesFertizone Product Catalog-14.03.22haitham ameenNo ratings yet
- Antibacterial Activity of Phyto Essential Oils On Flaccherie Causing Bacteria in The Mulberry Silk Worm, B.Mori. LDocument5 pagesAntibacterial Activity of Phyto Essential Oils On Flaccherie Causing Bacteria in The Mulberry Silk Worm, B.Mori. LIOSRjournalNo ratings yet
- Antimicrobial Activity of Leaf Extracts of Justicia Adhatoda L. in Comparison With VasicineDocument5 pagesAntimicrobial Activity of Leaf Extracts of Justicia Adhatoda L. in Comparison With VasicinelinubinoiNo ratings yet