You might also like
- Technical DatasheetsDocument6 pagesTechnical DatasheetsGaurang PatelNo ratings yet
- Earthing MaterialDocument1 pageEarthing MaterialGaurang PatelNo ratings yet
- Jual GPS Geodetik Topcon GR5 HUB 08111390801Document4 pagesJual GPS Geodetik Topcon GR5 HUB 08111390801AbieNo ratings yet
- Chapter 8.2-A Commissioning of The Micom P220 RelayDocument22 pagesChapter 8.2-A Commissioning of The Micom P220 RelayGaurang PatelNo ratings yet
- 7sa510 V3.2Document278 pages7sa510 V3.2anon_346282727No ratings yet
- Numerical Current Comparison Protection with Auto-ReclosureDocument196 pagesNumerical Current Comparison Protection with Auto-ReclosureGaurang PatelNo ratings yet
- Payslip For The Month of Sep.2017: Earnings Entitled Amt. Earned Amt. Deductions AmountDocument1 pagePayslip For The Month of Sep.2017: Earnings Entitled Amt. Earned Amt. Deductions AmountGaurang PatelNo ratings yet
- 7RW600 AnsiDocument216 pages7RW600 AnsiGaurang Patel100% (1)
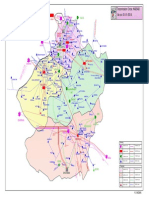
- Power Map of Eastern Region: BiharDocument1 pagePower Map of Eastern Region: Bihargaurang1111No ratings yet
- Testing A Metalenclosed Bus PDFDocument10 pagesTesting A Metalenclosed Bus PDFTunoNegro1No ratings yet
- Fire Protection ManualDocument82 pagesFire Protection ManualVivek SinghNo ratings yet
- 2016Document52 pages2016arvindNo ratings yet
- Earthing & Lightning Protection Calculations for ONGC Uran PlantDocument27 pagesEarthing & Lightning Protection Calculations for ONGC Uran Plantmahesh_sali200380% (5)
- Design 800kvDocument17 pagesDesign 800kvPriyesh GuptaNo ratings yet
- Failure Report GetcoDocument3 pagesFailure Report GetcoSanju GohilNo ratings yet
- Current Limiting Protector: For Systems Rated 2.8-38kV and Continuous Currents Through 5000ADocument8 pagesCurrent Limiting Protector: For Systems Rated 2.8-38kV and Continuous Currents Through 5000AhamiltonfabioborgesNo ratings yet
- Borivali CreekDocument3 pagesBorivali CreekGaurang PatelNo ratings yet
- Billiards XDocument2 pagesBilliards XGaurang PatelNo ratings yet
- Aluminum Seamless Bus PipeDocument2 pagesAluminum Seamless Bus PipeJose Carlos KnuppNo ratings yet
- Fatal Colonoscopy Due To Bowel PerforationDocument6 pagesFatal Colonoscopy Due To Bowel PerforationGaurang PatelNo ratings yet
- Billiards XDocument2 pagesBilliards XGaurang PatelNo ratings yet
- A Small Write Up On Working Experience at SLPP (Surat Lignite Power Project), GIPCLDocument6 pagesA Small Write Up On Working Experience at SLPP (Surat Lignite Power Project), GIPCLGaurang PatelNo ratings yet
- A Small Write Up On Working Experience at SLPP (Surat Lignite Power Project), GIPCLDocument6 pagesA Small Write Up On Working Experience at SLPP (Surat Lignite Power Project), GIPCLGaurang PatelNo ratings yet
- Risk of Colon Perforation During Colonoscopy at Baylor University Medical CenterDocument5 pagesRisk of Colon Perforation During Colonoscopy at Baylor University Medical CenterGaurang PatelNo ratings yet
- A Small Write Up On Working Experience at SLPP (Surat Lignite Power Project), GIPCLDocument6 pagesA Small Write Up On Working Experience at SLPP (Surat Lignite Power Project), GIPCLGaurang PatelNo ratings yet
- Chess AnimationDocument3 pagesChess Animationyogbal_animaNo ratings yet
- Chopper ChallengeDocument2 pagesChopper ChallengeGaurang PatelNo ratings yet
- Transmission Circle: NADIAD As On: 01-01-2014: Gandhi NagarDocument1 pageTransmission Circle: NADIAD As On: 01-01-2014: Gandhi NagarGaurang PatelNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The artery most likely to be eroded in perforation of the posterior wall of the first part of the duodenum is the superior pancreaticoduodenal artery. It is a branch of the gastroduodenal arteryDocument33 pagesThe artery most likely to be eroded in perforation of the posterior wall of the first part of the duodenum is the superior pancreaticoduodenal artery. It is a branch of the gastroduodenal arteryWahida Amalin Ab RazakNo ratings yet
- Sample: Ventral Hernia RepairDocument8 pagesSample: Ventral Hernia RepairInggriht Senny BondangNo ratings yet
- Pilates For SwimmersDocument10 pagesPilates For SwimmersMickNo ratings yet
- Joseph Pilates - 34 Classic Mat Exercises - LongversionDocument11 pagesJoseph Pilates - 34 Classic Mat Exercises - Longversionmxpxaxo100% (1)
- Pediatrics surgery I: Infantile hypertrophic pyloric stenosis and malrotationDocument24 pagesPediatrics surgery I: Infantile hypertrophic pyloric stenosis and malrotationMalueth AnguiNo ratings yet
- Where Does Digestion Begin?: Questions and AnswersDocument10 pagesWhere Does Digestion Begin?: Questions and AnswersJosefitaNo ratings yet
- Appendicitis: Ahmednagar Homoeopathic Medical College & Hospital AhmednagarDocument13 pagesAppendicitis: Ahmednagar Homoeopathic Medical College & Hospital AhmednagarSuhas IngaleNo ratings yet
- Acute and Chronic CholecystitisDocument10 pagesAcute and Chronic Cholecystitisissam_1994No ratings yet
- All Yoga PosesDocument24 pagesAll Yoga PosesBiljana GolicNo ratings yet
- Self Care Handout-1Document3 pagesSelf Care Handout-1Wandarh RhNo ratings yet
- Urinary System15Document47 pagesUrinary System15Michael John PaderesNo ratings yet
- CC Assignment2ndsem PalayDocument2 pagesCC Assignment2ndsem PalayRalph AJ BalmesNo ratings yet
- What Is Abdominal Pain? TreatmentDocument2 pagesWhat Is Abdominal Pain? TreatmentErick YohanesNo ratings yet
- Multi-Orgasmic Man - Exercises To Become A Multi-Orgasmic - Wen, Feng - 2016 - Anna's ArchiveDocument26 pagesMulti-Orgasmic Man - Exercises To Become A Multi-Orgasmic - Wen, Feng - 2016 - Anna's ArchiveShivam VishwaNo ratings yet
- Medical Terminology Terms ReviewDocument23 pagesMedical Terminology Terms ReviewQum ArNo ratings yet
- A. 2019. 07. Peritoneum DPTDocument39 pagesA. 2019. 07. Peritoneum DPTAzhar Ahmed SoomroNo ratings yet
- Abdominal Incision Types and Selection GuideDocument3 pagesAbdominal Incision Types and Selection GuidekukadiyaNo ratings yet
- Jurnal Hiperfosfat 2Document5 pagesJurnal Hiperfosfat 2Anggie Pradetya MaharaniNo ratings yet
- Is Baar Sabka Achha HogaDocument29 pagesIs Baar Sabka Achha HogasurajmotwaniNo ratings yet
- Pneumo PeritoneumDocument31 pagesPneumo PeritoneumRaif RizqullahNo ratings yet
- Working out and eating right at home with bodyweight exercises for a weekDocument3 pagesWorking out and eating right at home with bodyweight exercises for a weektomorrow x togetherNo ratings yet
- Functions of Bile Salts: Emulsification, Absorption of Fats and Fat-Soluble VitaminsDocument24 pagesFunctions of Bile Salts: Emulsification, Absorption of Fats and Fat-Soluble VitaminsAyeshaNo ratings yet
- 14 Inner and Outer Core ExercisesDocument17 pages14 Inner and Outer Core ExercisesАлексей СеменовNo ratings yet
- Digestive SystemDocument8 pagesDigestive SystemKeith Dion FacundoNo ratings yet
- Kidney QuizDocument3 pagesKidney QuizBindashboy0100% (1)
- Test Bank For Comprehensive Radiographic Pathology 5th Edition EisenbergDocument17 pagesTest Bank For Comprehensive Radiographic Pathology 5th Edition EisenbergValerieTaylorptszg100% (79)
- VULNUS ICTUM IN ABDOMENDocument19 pagesVULNUS ICTUM IN ABDOMENHardyanti DahlanNo ratings yet
- Classic Autopsy TechniquesDocument27 pagesClassic Autopsy TechniquesYenny BelindaNo ratings yet
- Aeshna (Hesperaeschna) Cornigera Planaltica (Odonata: Aeshnidae)Document6 pagesAeshna (Hesperaeschna) Cornigera Planaltica (Odonata: Aeshnidae)juan pablo zuluaga montoyaNo ratings yet
- 5 DNSA Treatment PDFDocument9 pages5 DNSA Treatment PDFklinik bapelkes ksNo ratings yet