Professional Documents
Culture Documents
Assessing The Reliability and Validity of A.4
Uploaded by
qonitaOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Assessing The Reliability and Validity of A.4
Uploaded by
qonitaCopyright:
Available Formats
Research Report
Assessing the Reliability and Validity of
a Shorter Walk Test Compared With the
10-Meter Walk Test for Measurements of Gait
Speed in Healthy, Older Adults
Denise M. Peters, DPT1; Stacy L. Fritz, PT, PhD2; Debra E. Krotish, PhD1
ABSTRACT ment of walking speed when using it as a 1-time indicator of
Background and Purpose: Walking speed is associated with health status.
several health-related outcomes. Research examining how Key Words: older adult, gait speed, measurement, reliability,
differences in test walking distance affect walking speed validity
reliability and validity is limited. The primary purpose of this
study was to examine the reliability and concurrent validity of (J Geriatr Phys Ther 2013;36:24-30.)
gait speed measurements obtained from a 4-Meter Walk Test
compared with the commonly used 10-Meter Walk Test. A INTRODUCTION
second objective was to similarly examine 2 different timing
methods: stopwatch and automatic timers.
Walking speed is an important aspect of gait and is com-
Methods: Forty-three healthy, older adults (mean age 84.3
6.9 years) performed 3 consecutive walking trials on the 4- monly used as an objective measure of functional mobility
and 10-Meter Walk Tests at their self-selected walking speed. in both clinical and research settings. Its importance lies
Results: Gait speed measurements for both tests were shown not only in its implications for community ambulation but
to have excellent test-retest reliability (ICC values of 0.96- also because of its relationship to various health outcomes.
0.98), with similar results for stopwatch and automatic timer
Walking speed has been shown to be a key factor in deter-
assessments (ICC values of 0.99-1.00). Standard error of the
measurement (SEM) values were small (0.004-0.008 m/s) mining rehabilitation needs1,2 and discharge location3 and
across measurement methods. While the ICC value for gait has the potential to predict future functional decline4,5
speed measurements between the 2 walk tests was 0.93, the and fall risk.6,7 Furthermore, a decline in walking speed
Bland-Altman analysis revealed a discrepancy of 0.15 to is associated with several health-related factors such as
0.17 m/s between measurement methods.
disability, hospitalization, loss of independence, and mor-
Discussion: Both 4- and 10-m gait speed assessments had
excellent test-retest reliability with similar SEM and minimal tality.8-11 Improvement in walking speed has been linked
detectable change values. There was little difference in SEM to constructive changes in quality of life12 and walking
values between the 2 timing methods. While the mean differ- behavior.13 This importance, combined with its ease of use
ence in gait speed between the 4- and 10-Meter Walk Tests and objectivity, substantiates the use of walking speed as a
was small, the range of the measurement differences was
practical clinical measure that offers more insight into an
large enough to potentially mask meaningful changes in gait
speed over time if both methods were used interchangeably. individuals overall functional capacity.
Conclusions: While the reliability of both walking tests is excel- Walking speed can be quickly and easily assessed in most
lent, the 4-Meter Walk Test does not exhibit a high enough clinical and research settings, and measurements of walking
degree of concurrent validity with the 10-Meter Walk Test speed have demonstrated good reliability across multiple
to be used interchangeably for gait speed assessments in
patient populations and in individuals with known gait
healthy, older adults. We therefore recommend using the
10-Meter Walk Test to obtain the most valid clinical assess- impairments.14-16 Great variation exists, however, in mea-
surement methods used to assess walking speed. There is
1Department little consensus concerning optimal testing parameters such
of Exercise Science, University of South
Carolina, Columbia. as starting protocol, pace, and timed walking distance. Often
2Palmetto Health, Division of Geriatrics, Columbia, South tests are chosen based more on tester preference and conve-
Carolina. nience, especially in clinical settings where space is limited.
There are no conflicts of interest, and no external funding The 10-Meter Walk Test is a commonly used measure
was used for this study. for assessing walking speed.17-22 It requires a 20-m path that
Address correspondence to: Denise M. Peters, DPT, includes 5 m for acceleration and deceleration. Practically,
Department of Exercise Science, University of South however, a full 20-m walkway is not always available, so
Carolina, 921 Assembly St, 3rd Floor PHRC, Columbia, SC there are several shorter distances commonly used to assess
29208 (petersd20@gmail.com). walking speed including 3-, 4-, and 6-m assessments.23
DOI: 10.1519/JPT.0b013e318248e20d Two studies with neurologic populations found significant
24 Volume 36 Number 1 January-March 2013
Copyright 2013 The Section on Geriatrics of the American Physical Therapy Association. Unauthorized reproduction of this article is prohibited.
JPT200142.indd 24 12/7/12 7:21 PM
Research Report
differences in fast walking speed between 5- and 10-m test
distances,24 and in self-selected walking speed between
10 m and real-life environments (eg, parking lot of a
shopping center).25 Overall, however, research examining
how subtle differences in test walking distance affect gait
speed reliability and validity is limited both within and
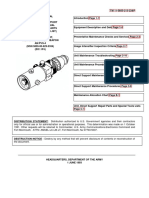
across patient populations. It is unclear whether shorter Figure 1. Outline of the 4- and 10-Meter Walk Tests.
test walking distances provide as accurate, representative
assessments of walking speed as longer distances. conditions was randomly varied among participants so
The primary purpose of this study was to examine that not all participants were performing the longer walk-
the validity of a 4-Meter Walk Test compared with the ing test at the end of the testing session. Participants were
commonly used 10-Meter Walk Test when used to assess instructed to walk at your comfortable, usual pace until
walking speed in healthy, older adults. An additional objec- they reached the end of the marked path. Wireless timers
tive was to examine the reliability and validity of walking (Brower Timing Systems) that send radio transmissions
speed measurements obtained through 2 different methods: were used to record walking time. These timers were
the use of a stopwatch and automatic timers. If reliable, placed at the beginning and end of the timed walkway
representative assessments of gait speed can be achieved area and automatically started/stopped as the participant
using shorter distances with a handheld timer, this might walked past them. In addition, a member of the research
increase the use of walking speed measurements in clinical
team simultaneously measured walking time with a stop-
settings, thereby offering more insight into an individuals
watch, starting the stopwatch as soon as the participants
functional health status and imparting clinically meaning
lead leg (or assistive device) crossed the first marker and
information to help guide and monitor patient treatment.
stopping it when the participants lead leg (or assistive
Although reliability assessments across longer time inter-
vals is more applicable for clinical outcomes, intrasession device) crossed the second marker. The same person per-
reliability is an important first step to determine reliability formed all stopwatch measurements to prevent introduc-
of a measurement without external influences (eg, time) ing interrater variability. Participants were provided rest
and is appropriate for 1-time assessments such as when breaks as needed throughout the testing session.
using walking speed as a vital sign.26
Data Analysis
The Shapiro-Wilks test was used to test for normality of
METHODS
data. Intraclass correlation coefficients (ICC3,1) were calcu-
Design and Participants lated to examine the reliability of gait speed measurements
A cross-sectional study design was used with comparisons across walking trials 2 and 3 for the 4- and 10-Meter Walk
of gait speed between 2 different walking tests. Forty-three Tests for both stopwatch and automatic timer assessments.
participants were recruited from a local retirement com-
The ICC values were interpreted using the benchmarks
munity. Inclusion criteria included age 65 years or older,
suggested by Menz et al28: more than 0.75 excellent reli-
the ability to reliably follow 2-step instructions, and the
ability; 0.40 to 0.75 fair to good reliability; and less than
ability to walk 20 m with or without an assistive device.
0.40 poor reliability. To quantify the amount of change
Exclusion criteria included severe weight-bearing pain
(rated 5/10 on the visual analog pain scale), severe visual in gait speed that must be observed to be considered to
impairment, and/or severe arthritis or orthopedic prob- exceed measurement error and variability, the minimal
lems that limited ambulation ability. All participants gave detectable change (MDC) was calculated at both the 90%
written informed consent. The study was approved by the and 95% confidence levels using the following formulas:
institutional review board at Palmetto Health. MDC90 1.64 SEM 2 and MDC95 1.96 SEM
2, where SEM is standard error of measurement. The
Walking Procedure and Measurement SEM value was determined using the formula [SD (1
Walking speed was assessed at participants self-selected r)], where r is the test-retest reliability coefficient (in this
walking pace using a 4-Meter Walk Test (with 2 m pro- case, ICC3,1) and SD is the standard deviation of the trial
vided for acceleration/deceleration) and the 10-Meter difference scores.29,30 The SEM is the estimated standard
Walk Test (with 5 m provided for acceleration/decelera- deviation of measurement error, or the difference between
tion) (Figure 1). Distances were provided at the beginning the observed values and the true values. The SEM was
and end of the timed walkway to allow participants multiplied by 1.64 or 1.96 to reflect the 90% or 95%
space to accelerate/decelerate outside the data collection confidence intervals (CIs), respectively. This value was
area to help reduce gait variability introduced during multiplied by the square root of 2 to account for the error
these phases.23,27 Each participant completed 3 consecu- associated with repeat measurements.29,31
tive trials for each walking test, for a total of 6 walking The agreement between stopwatch and automatic timer
trials. Order of administration of the 2 different walking assessments (for both the 4- and 10-Meter Walk Tests)
Journal of GERIATRIC Physical Therapy 25
Copyright 2013 The Section on Geriatrics of the American Physical Therapy Association. Unauthorized reproduction of this article is prohibited.
JPT200142.indd 25 12/7/12 7:21 PM
Research Report
and between 4- and 10-m gait speed assessments was
MDC95
examined using ICC2,1 and the Bland-Altman method32
0.02
0.02
(95% limits of agreement), with similar interpretation of
ICC point estimates as previously described. Validity was
examined for both single trial (second walking trial) and
MDC90
0.02
0.01
average (across all 3 walking trials) gait speed assessments.
The Bland-Altman technique allows one to visually assess
the agreement between 4- and 10-m gait speed assessments
0.008
0.006
SEM
(or between stopwatch and automatic timer assessments)
by plotting the difference in the measurement methods
4-m Walk, m/s
against the mean of the 2 measurements.32,33 The result-
0.96 (0.94-0.98)
0.97 (0.95-0.99)
ICC (95% CI)
ing plot shows the size and range of the measurement
Abbreviations: CI, confidence interval; ICC, intraclass correlation coefficient; MDC90, minimal detectable change at 90% CI; MDC95, minimal detectable change at 95% CI; SEM, standard error of measurement.
differences and their distribution around the mean. The
95% limits of agreement (mean difference 1.96 SD of
the differences between measurement methods) provide
an indication of how far apart measurements by the
0.97 (0.23)
0.97 (0.23)
2 walking tests (or 2 timing methods) are likely to be for
Trial 3b
most individuals. 34 A smaller range between these 2 limits
indicates a better level of agreement, and how close the
measurements have to be is a clinical question/decision (is
0.97 (0.22)
0.97 (0.22)
the discrepancy between methods large enough to mean-
Trial 2b
ingfully affect the interpretation of results?), not based on
statistical testing. When comparing the 2 timing methods,
single-trial assessments of walking speed were used in the
Bland-Altman analyses. When comparing 4- and 10-m
MDC95
0.01
0.01
gait speed assessments, stopwatch assessments of walking
speed were used for the Bland-Altman analyses, as this
Table. Test-Retest Reliability of Gait Speed Measurements Across Consecutive Walking Trialsa
from of measurement has more clinical utility than auto-
matic timers. In addition, paired t tests were performed to
MDC90
0.01
0.01
test for systematic differences in gait speed between the
2 walk tests, with .05. All statistical analyses were
conducted using PASW version 18.0 (SPSS, Chicago, IL).
0.005
0.004
SEM
RESULTS
10-m Walk, m/s
Forty-three community-dwelling older adults (32 women,
11 men) with a mean age 84.3 years (SD 6.9) participated
0.98 (0.96-0.99)
0.98 (0.96-0.99)
ICC (95% CI)
in the study. Average walking speed (across all 3 trials) on
the 10-Meter Walk Test varied between 0.50 and 1.43 m/s,
with a mean walking speed of 0.96 m/s (SD 0.23) per
stopwatch assessment. Seven participants used an assis-
tive device for ambulation. One participant was unable to
0.98 (0.24)
0.98 (0.23)
complete a third ambulation trial due to personal time con-
Trial 3b
straints, so reliability analyses were performed and walking
aAll values except ICC values are expressed in m/s.
speed/time was averaged across the first 2 trials for this
participant. The Shapiro-Wilks test showed that gait speed
bGait speed values expressed as mean (SD).
0.97 (0.22)
0.97 (0.22)
measurements were normally distributed.
Trial 2b
Reliability Across Walking Trials
Both 4- and 10-m gait speed measurements were shown to
Automatic timer
have excellent test-retest reliability, with ICC values ranging
from 0.96 to 0.98 (Table). Reliability was similar for both
Stopwatch
stopwatch and automatic timer assessments, with SEM
values between 0.004 and 0.008 m/s and MDC90/MDC95
values between 0.01 and 0.02 m/s.
26 Volume 36 Number 1 January-March 2013
Copyright 2013 The Section on Geriatrics of the American Physical Therapy Association. Unauthorized reproduction of this article is prohibited.
JPT200142.indd 26 12/7/12 7:21 PM
Research Report
Validity of Stopwatch Measurements Compared With trial (P .957) or average (P .349) gait speed compari-
Automatic Timer sons. When comparing the second ambulation trial, both
Agreement between the 2 timing methods was excellent the 4- and 10-Meter Walk Test resulted in a mean gait
for both walking tests, with ICC values ranging from 0.99 speed value of 0.97 m/s (SD 0.22). When examining
(95% CI: 0.988-0.996) to 1.00 (95% CI: 0.999-1.00). average gait speed across the 2 tests, the 10-Meter Walk
The values for ICC were similar for both single-trial and Test resulted in a mean gait speed value of 0.96 m/s (SD
average gait speed assessments. Figure 2 shows a Bland- 0.23) compared with 0.95 m/s (SD 0.22) for the 4-Meter
Altman plot for the differences in gait speed between the Walk Test.
2 timing methods. While no obvious relationship between The ICC value for single-trial gait speed measurements
the difference and mean was observed for stopwatch and between the 4- and 10-Meter Walk Tests was 0.93 (95%
automatic timer assessments, there was a slightly better CI: 0.87-0.96) and for average gait speed measurements
level of agreement between the 2 timing methods on the was 0.93 (95% CI: 0.88-0.96). Figure 3 shows a Bland-
10-Meter Walk Test (95% limits of agreement ranged Altman plot for the differences in gait speed between the
from 0.02 to 0.02 m/s) than on the 4-Meter Walk Test 2 walking tests. No obvious relationship between the
(95% limits of agreement ranged from 0.05 to 0.05 difference and the mean was observed for 4- and 10-m
m/s). gait speed assessments, with similar mean differences and
95% limits of agreement noted for both single-trial (mean
Validity of 4- and 10-m Stopwatch Assessments of difference: 0.0007 m/s; 95% limits of agreement: 0.17
Gait Speed to 0.17 m/s) and average (mean difference: 0.0118 m/s;
Gait speed measurements were not significantly different 95% limits of agreement: 0.17 to 0.15 m/s) gait speed
between 4- and 10-m walk assessments for either single- comparisons.
Figure 2. Bland-Altman plots representing comparisons Figure 3. Bland-Altman plots representing comparisons
between stopwatch (SW) and automatic timer single-trial between 4- and 10-m gait speed assessments obtained
gait speed assessments for the 4-Meter Walk Test (A) and using a stopwatch for single-trial (A) and average (B) gait
10-Meter Walk Test (B). The solid line represents the mean speeds. The solid line represents the mean difference in
difference in gait speed between the 2 timing methods, gait speed between the 2 walking tests, with the dashed
with the dashed lines representing the upper and lower lines representing the upper and lower 95% limits of
95% limits of agreement, mean 2 (SD). agreement, mean 2 (SD).
Journal of GERIATRIC Physical Therapy 27
Copyright 2013 The Section on Geriatrics of the American Physical Therapy Association. Unauthorized reproduction of this article is prohibited.
JPT200142.indd 27 12/7/12 7:21 PM
Research Report
DISCUSSION determination of whether 2 methods of clinical measure-
The use of automatic timers to record walking time is sim- ment agree sufficiently for them to be used interchange-
ple, but few clinical settings have such devices. Stopwatches, ably, or one in place of the other.32,33 The 2 methods may
on the contrary, are a more accessible instrument and often be used interchangeably if the calculated 95% limits of
used in both clinical and research settings to record walking agreement are close enough, per clinical decision, such that
time for calculations of gait speed across various distances. a difference between measurement methods as extreme as
Our results indicate excellent agreement both within and described by the limits of agreement would not meaning-
between stopwatch and automatic timer assessments across fully affect interpretation of results.32,34 The ICC values
2 different walking distances (4 and 10 m) in healthy, older for our data (0.93) indicated excellent agreement between
adults, with little difference in SEM values between the 2 4- and 10-m walking speed assessments, as mean gait
timing methods. Our ICC values were on the upper end of speed values differed by just 0.0007 m/s (SD 0.09) and
similar studies (ICC values from 0.88 to 0.97) that have 0.0118 m/s (SD 0.08) for single-trial and average gait
examined the reliability of gait speed measurements in this speed assessments, respectively, with slightly higher gait
patient population.15,35,36 Furthermore, the Bland-Altman speed values obtained with the 10-Meter Walk Test. While
analysis displayed a small range between the 95% limits the mean difference in gait speed between the 2 measures
of agreement (0.05 m/s or less), indicating a clinically was small, the range of the upper and lower 95% limits
acceptable degree of agreement such that the use of one of agreement was 0.15 to 0.17 m/s. Several studies
timing method over the other would not meaningfully have demonstrated 0.08 to 0.14 m/s as the needed change
affect interpretation of gait speed results. for a meaningful improvement in walking speed in older
If walking speed is to be used as a vital sign in health adults.9,17,37 In addition, improvements in walking speed
care assessments, measurement methods associated with a of 0.1 m/s or more have been shown to be a useful pre-
small SEM value are important to ensure a small degree of dictor for well-being whereas decreases in walking speed
measurement error when assessing baseline values. Both of the same amount have been linked with poorer health
4- and 10-m gait speed assessments had excellent test-retest outcomes.26 Given these values of meaningful change in
reliability, with similar SEM values when examined across gait speed, the calculated limits of agreement in our study
consecutive walking trials. For example, if an individual indicate that the degree of agreement between 4- and 10-m
exhibited a gait speed of 0.98 m/s on the 10-Meter Walk gait speed assessments is not sufficient to permit using
Test, our results indicate that we could be 95% confident the 2 walking tests interchangeably in assessments of gait
that this individuals true gait speed is between 0.97 and speed in healthy, older adults. The discrepancy between
0.99 m/s, or 2 times the SEM (0.005 m/s for stopwatch measurement methods is large enough to potentially mask
assessments); similarly, if the 4-Meter Walk Test was used meaningful changes in gait speed over time if both meth-
as a screening tool, our results indicate that we could be ods are used. Therefore, although the reliability of both
95% confident that this individuals true gait speed is walking tests is excellent, the 4-Meter Walk Test does not
between 0.96 and 1.00 m/s. exhibit a high enough degree of concurrent validity with
Another extrapolation is to look at gait speed changes the 10-Meter Walk Test to be used interchangeably for gait
over time (eg, from pre- to posttreatment). Our results speed assessments in healthy, older adults.
indicate that a change in gait speed of 0.01 m/s or more or This study is one of the few to investigate how subtle
0.02 m/s or more is necessary for 10- and 4-m walk assess- differences in test walking distance affect the validity of
ments, respectively, to be 95% confident that a true change walking speed assessments. We did not attempt, how-
has occurred beyond measurement error in healthy, older ever, to investigate the reliability and validity of different
adults. As several participants required an assistive device walking speed assessments in specific patient populations,
to walk, future research work could examine measure- which has been the focus of previous research.24,25 Our
ment reliability and determine MDC values specific to this results indicate that although reliable assessments of walk-
subpopulation of individuals. Furthermore, MDC values ing speed in healthy, older adults can be obtained using
calculated from measurements taken across longer time a 4-Meter Walk Test, 4-m walking speed assessments
intervals, such as days or weeks, could be in a manner dif- cannot be used interchangeably with 10-Meter Walk Test
ferent from those that are calculated from repeat measure- assessments. Consideration must be taken when viewing
ments taken within the same testing session. our results, however, as they may have been influenced
Examining the validity of a shorter walk test compared by a number of limitations present in this study. First, our
with the commonly used 10-Meter Walk Test when deter- study sample was relatively small, and it is possible that a
mining gait speed is important, as space is often a limiting lesser discrepancy between measurement methods might
factor in clinical settings. While the ICC value quantifies the have been observed with a larger sample size. Furthermore,
reliability of 2 methods, it alone is insufficient to evaluate our sample included both individuals who ambulated with
patterns of discrepancy that may be present among differ- and without an assistive device, which improves external
ences in the data. The Bland-Altman method aids in the validity but increases variability in sample characteristics.
28 Volume 36 Number 1 January-March 2013
Copyright 2013 The Section on Geriatrics of the American Physical Therapy Association. Unauthorized reproduction of this article is prohibited.
JPT200142.indd 28 12/7/12 7:21 PM
Research Report
Future studies with a larger number of individuals who use 3. Rabadi MH, Blau A. Admission ambulation velocity predicts length of stay
and discharge disposition following stroke in an acute rehabilitation hospital.
an assistive device could examine measurement reliability Neurorehabil Neural Repair. 2005;19(1):20-26.
and validity in this subpopulation. In addition, the stabil- 4. Montero-Odasso M, Schapira M, Soriano ER, et al. Gait velocity as a single
predictor of adverse events in healthy seniors aged 75 years and older.
ity of gait speed measurements over time was not assessed J Gerontol A Biol Sci Med Sci. 2005;60(10):1304-1309.
in this study; reliability and validity analyses among gait 5. Brach JS, VanSwearingen JM, Newman AB, Kriska AM. Identifying early
decline of physical function in community-dwelling older women: performance-
speed measurements based on walking trials performed on based and self-report measures. Phys Ther. 2002;82(4):320-328.
separate days may result in different ICC and MDC values 6. Maki BE. Gait changes in older adults: predictors of falls or indicators of fear.
J Am Geriatr Soc. 1997;45(3):313-320.
than the current study. Intrasession reliability needs to 7. de Rekeneire N, Visser M, Peila R, et al. Is a fall just a fall: correlates of falling
be assessed first, however, to decrease possible variations in healthy older persons. The Health, Aging and Body Composition Study. J
Am Geriatr Soc. 2003;51(6):841-846.
from external influences, followed by reliability evalua- 8. Studenski S, Perera S, Wallace D, et al. Physical performance measures in
tions across longer time intervals. Also, the participants in the clinical setting. J Am Geriatr Soc. 2003;51(3):314-322.
9. Hardy SE, Perera S, Roumani YF, Chandler JM, Studenski SA. Improvement
our study were all relatively healthy, older adults with a in usual gait speed predicts better survival in older adults. J Am Geriatr Soc.
mean self-selected walking speed of 0.96 m/s (SD 0.23), 2007;55(11):1727-1734.
10. Kuo HK, Leveille SG, Yen CJ, et al. Exploring how peak leg power and
which is similar to 8,20 or somewhat lower15,36,38 than gait usual gait speed are linked to late-life disability: data from the National Health
speed values obtained from other studies examining walk- and Nutrition Examination Survey (NHANES), 1999-2002. Am J Phys Med
Rehabil. 2006;85(8):650-658.
ing speed in older adults. These results might be different 11. Penninx BW, Ferrucci L, Leveille SG, Rantanen T, Pahor M, Guralnik
for older adults who ambulate at slower or faster walking JM. Lower extremity performance in nondisabled older persons as a predictor
of subsequent hospitalization. J Gerontol A Biol Sci Med Sci. 2000;55(11):
speeds and/or who have specific pathologies (eg, stroke). M691-M697.
Finally, although the differences in gait speed measure- 12. Schmid A, Duncan PW, Studenski S, et al. Improvements in speed-based gait
classifications are meaningful. Stroke. 2007;38(7):2096-2100.
ments between the 4- and 10-Meter Walk Tests greatly 13. Bowden MG, Balasubramanian CK, Behrman AL, Kautz SA. Validation
exceeded the MDC values of the current study (0.01-0.02 of a speed-based classification system using quantitative measures of walking
performance poststroke. Neurorehabil Neural Repair. 2008;22(6):672-675.
m/s), we considered MDC values from other studies to 14. Green J, Forster A, Young J. Reliability of gait speed measured by a
strengthen our conclusions; however, the amount of change timed walking test in patients one year after stroke. Clin Rehabil. 2002;16(3):
306-314.
that is considered meaningful by other studies may not 15. Steffen TM, Hacker TA, Mollinger L. Age- and gender-related test
really be meaningful if these values did not exceed measure- performance in community-dwelling elderly people: Six-Minute Walk Test, Berg
Balance Scale, Timed Up & Go Test, and gait speeds. Phys Ther. 2002;82(2):
ment error and variability. 128-137.
16. van Loo MA, Moseley AM, Bosman JM, de Bie RA, Hassett L. Test-
re-test reliability of walking speed, step length and step width measurement
CONCLUSIONS after traumatic brain injury: a pilot study. Brain Inj. 2004;18(10):1041-1048.
Although 4- and 10-m walking speed assessments in 17. Perera S, Mody SH, Woodman RC, Studenski SA. Meaningful change and
responsiveness in common physical performance measures in older adults.
healthy, older adults demonstrated excellent test-retest J Am Geriatr Soc. 2006;54(5):743-749.
reliability and were highly correlated, our results indicate 18. Ota A, Yasuda N, Horikawa S, Fujimura T, Ohara H. Differential effects
of power rehabilitation on physical performance and higher-level functional
that there is insufficient agreement between the 2 walk- capacity among community-dwelling older adults with a slight degree of frailty.
ing tests to permit them to be used interchangeably in this J Epidemiol. 2007;17(2):61-67.
19. Avlund K, Rantanen T, Schroll M. Tiredness and subsequent disability in
patient population. We therefore recommend the use of older adults: the role of walking limitations. J Gerontol A Biol Sci Med Sci.
the 10-Meter Walk Test to obtain the most valid clinical 2006;61(11):1201-1205.
assessment of walking speed in healthy, older adults; how- 20. Kressig RW, Wolf SL, Sattin RW, et al. Associations of demographic,
functional, and behavioral characteristics with activity-related fear of
ever, a 4-Meter Walk Test can be used if space is a limiting falling among older adults transitioning to frailty. J Am Geriatr Soc.
factor, but the same walking test needs to be used for all 2001;49(11):1456-1462.
21. van Hedel HJ, Dietz V, Curt A. Assessment of walking speed and
subsequent measurements of gait speed for evaluations of distance in subjects with an incomplete spinal cord injury. Neurorehabil
meaningful change in gait speed over time. Our results also Neural Repair. 2007;21(4):295-301.
22. Jorgensen JR, Bech-Pedersen DT, Zeeman P, Sorensen J, Andersen
demonstrated that handheld stopwatches were as reliable LL, Schonberger M. Effect of intensive outpatient physical training on gait
as automatic timers in measurements of gait speed. Further performance and cardiovascular health in people with hemiparesis after
stroke. Phys Ther. 2010;90(4):527-537.
research should continue to examine how subtle differences 23. Graham JE, Ostir GV, Fisher SR, Ottenbacher KJ. Assessing walking
in walking test parameters affect walking speed assessments speed in clinical research: a systematic review. J Eval Clin Pract. 2008;14(4):
across different patient populations. If a shorter walking 552-562.
24. Salbach NM, Mayo NE, Higgins J, Ahmed S, Finch LE, Richards
test can provide a high, clinically acceptable degree of agree- CL. Responsiveness and predictability of gait speed and other disability
ment of gait speed measures compared with the 10-Meter measures in acute stroke. Arch Phys Med Rehabil. 2001;82(9):1204-1212.
25. Moseley AM, Lanzarone S, Bosman JM, et al. Ecological validity of
Walk Test, this might increase the use of walking speed walking speed assessment after traumatic brain injury: a pilot study. J Head
measurements in clinical settings to offer more insight into Trauma Rehabil. 2004;19(4):341-348.
26. Fritz S, Lusardi M. White paper: walking speed: the sixth vital sign.
a patients functional mobility and health status. J Geriatr Phys Ther. 2009;32(2):2-5.
27. Lindemann U, Najafi B, Zijlstra W, et al. Distance to achieve steady
state walking speed in frail elderly persons. Gait Posture. 2008;27(1):91-96.
REFERENCES 28. Menz HB, Latt MD, Tiedemann A, Mun San Kwan M, Lord SR.
1. Purser JL, Weinberger M, Cohen HJ, et al. Walking speed predicts health Reliability of the GAITRite walkway system for the quantification of temporo-
status and hospital costs for frail elderly male veterans. J Rehabil Res Dev. spatial parameters of gait in young and older people. Gait Posture. 2004;20(1):
2005;42(4):535-546. 20-25.
2. Goldie PA, Matyas TA, Evans OM. Deficit and change in gait velocity during 29. Haley SM, Fragala-Pinkham MA. Interpreting change scores of tests
rehabilitation after stroke. Arch Phys Med Rehabil. 1996;77(10):1074-1082. and measures used in physical therapy. Phys Ther. 2006;86(5):735-743.
Journal of GERIATRIC Physical Therapy 29
Copyright 2013 The Section on Geriatrics of the American Physical Therapy Association. Unauthorized reproduction of this article is prohibited.
JPT200142.indd 29 12/7/12 7:21 PM
Research Report
30. Fritz SL, Blanton S, Uswatte G, Taub E, Wolf SL. Minimal detectable change values and correlates for older adults. J Orthop Sports Phys Ther. 1996;24(2):
scores for the Wolf Motor Function Test. Neurorehabil Neural Repair. 86-90.
2009;237:662-667. 36. Hollman JH, Childs KB, McNeil ML, Mueller AC, Quilter CM, Youdas
31. Wyrwich KW, Tierney WM, Wolinsky FD. Further evidence supporting JW. Number of strides required for reliable measurements of pace, rhythm
an SEM-based criterion for identifying meaningful intra-individual changes in and variability parameters of gait during normal and dual task walking in older
health-related quality of life. J Clin Epidemiol. 1999;52(9):861-873. individuals. Gait Posture. 2010;32(1):23-28.
32. Bland JM, Altman DG. Statistical methods for assessing agreement between two 37. Kwon S, Perera S, Pahor M, et al. What is a meaningful change in
methods of clinical measurement. Lancet. 1986;1(8476):307-310. physical performance? Findings from a clinical trial in older adults (the LIFE-P
33. Bland JM, Altman DG. Measuring agreement in method comparison study). J Nutr Health Aging. 2009;13(6):538-544.
studies. Stat Methods Med Res. 1999;8(2):135-160. 38. Cesari M, Kritchevsky SB, Penninx BW, et al. Prognostic value of
34. Bland JM, Altman DG. Comparing methods of measurement: why plotting difference usual gait speed in well-functioning older peopleresults from the Health,
against standard method is misleading. Lancet. 1995;346(8982):1085-1087. Aging and Body Composition Study. J Am Geriatr Soc. 2005;53(10):
35. Bohannon RW, Andrews AW, Thomas MW. Walking speed: reference 1675-1680.
Call for Reviewers
The Journal of Geriatric Physical Therapy is seeking to expand our cadre of manuscript reviewers.
Job Description:
Receive 4 - 5 manuscript per year for blinded peer review
Emphasis on quality of science: importance of research question, clarity of study design, appropriateness of analysis,
accuracy of interpretation of results
2-week turn around for review
Materials available at www.editorialmanager.com/jgpt
possible recommendations: reject, revise with additional revie w, minor revision, accept
provide confidential comments to editor
provide constructive criticism and suggestions to authors
follow reviewed manuscripts through revision process
develop review skills
Prerequisites:
Graduate Degree beyond entry level (e.g., PhD, EdD, DSc, or t-DPT)
Submission, revision, and acceptance of at least two manuscripts in a peer-reviewed journal
To Apply: please send letter of application highlighting research interests/experience and current CV to Michelle Lusardi,
PT, DPT, PhD, JGPT Editor at lusardim@sacredheart.edu
30 Volume 36 Number 1 January-March 2013
Copyright 2013 The Section on Geriatrics of the American Physical Therapy Association. Unauthorized reproduction of this article is prohibited.
JPT200142.indd 30 12/7/12 7:21 PM
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Briefings To University of Minnesota Board of Regents On Markingson CaseDocument288 pagesBriefings To University of Minnesota Board of Regents On Markingson CaseMarkingsonCaseNo ratings yet
- TM11-5855-213-23&P - AN-PVS4 - UNIT AND DIRECT SUPPORT MAINTENANCE MANUAL - 1 - June - 1993Document110 pagesTM11-5855-213-23&P - AN-PVS4 - UNIT AND DIRECT SUPPORT MAINTENANCE MANUAL - 1 - June - 1993hodhodhodsribd100% (1)
- Buddhism in AndhraDocument16 pagesBuddhism in AndhraRaghavendrarao ChukkaNo ratings yet
- National Conference: Indo Asian Academy Degree College Indo Asian Women'S Degree CollegeDocument2 pagesNational Conference: Indo Asian Academy Degree College Indo Asian Women'S Degree CollegeajaxNo ratings yet
- Measures of Central Tendency Ungrouped DataDocument4 pagesMeasures of Central Tendency Ungrouped DataLabLab ChattoNo ratings yet
- Standards Booklet For Igsce Sociology (0495)Document64 pagesStandards Booklet For Igsce Sociology (0495)Ingrit AgustinNo ratings yet
- Data Mining Chapter3 0Document32 pagesData Mining Chapter3 0silwalprabinNo ratings yet
- Lesson Plan in Story Time-C.o. 3Document9 pagesLesson Plan in Story Time-C.o. 3Girlie May MabasagNo ratings yet
- DesignationDocument21 pagesDesignationGayl Ignacio TolentinoNo ratings yet
- Simplified Remote Restart White PaperDocument33 pagesSimplified Remote Restart White Paperch herlinNo ratings yet
- Xii Practical Part B (2022-23) PDFDocument14 pagesXii Practical Part B (2022-23) PDFanshika goelNo ratings yet
- Deduccion LogicaDocument27 pagesDeduccion Logicamartin quezadaNo ratings yet
- B1 Writing Task Analytic RubricDocument1 pageB1 Writing Task Analytic RubricsecilerkollNo ratings yet
- MLA Short GuideDocument2 pagesMLA Short GuidekennethreedsNo ratings yet
- Health On The Net FoundationDocument4 pagesHealth On The Net FoundationmisanthropoNo ratings yet
- Infinity Meta Weekly Ot - Ka & TN - Non MPC & Other Subjects - SyllabusDocument2 pagesInfinity Meta Weekly Ot - Ka & TN - Non MPC & Other Subjects - SyllabusR PranavNo ratings yet
- 2-General Physics 1-Uncertainties in MeasurementDocument22 pages2-General Physics 1-Uncertainties in MeasurementLiza Macalinao MangalimanNo ratings yet
- Error DetailsDocument3 pagesError Detailsnaresh kumarNo ratings yet
- Anxiety in Practicing English Language As A Means of Communication in Esl ClassroomDocument40 pagesAnxiety in Practicing English Language As A Means of Communication in Esl Classroomkirovdust100% (1)
- KPO An Opportunity For CADocument5 pagesKPO An Opportunity For CApathan1990No ratings yet
- Signal System 50 Most Important MCQ With SolutionDocument14 pagesSignal System 50 Most Important MCQ With SolutionattiqueNo ratings yet
- Technical Note - Measurement MicrophonesDocument4 pagesTechnical Note - Measurement MicrophonesWillFonsecaNo ratings yet
- KitkatDocument11 pagesKitkatSugandha GuptaNo ratings yet
- Math 1220 Calculus 2 Final Sample 2 - Summer 01Document2 pagesMath 1220 Calculus 2 Final Sample 2 - Summer 01Tyler CameronNo ratings yet
- Aiyaz Sayed Khaiyum ThesisDocument5 pagesAiyaz Sayed Khaiyum Thesisafbtbakvk100% (2)
- Peran Lembaga Adat Melayu Lam Riau Dalam Pelestarian Budaya Daerah Di Provinsi RDocument9 pagesPeran Lembaga Adat Melayu Lam Riau Dalam Pelestarian Budaya Daerah Di Provinsi RRahmi nurhayatiNo ratings yet
- Analysis of The Trollaukin Bind.Document6 pagesAnalysis of The Trollaukin Bind.EdwardNo ratings yet
- Bei 076 III II AntenamarksDocument8 pagesBei 076 III II Antenamarksshankar bhandariNo ratings yet
- Install ElucidationDocument57 pagesInstall ElucidationAbomazen GalalNo ratings yet
- Chapter 9Document52 pagesChapter 9Navian NadeemNo ratings yet