You might also like
- USMLE 2020 Recall MR MurphyDocument42 pagesUSMLE 2020 Recall MR MurphyChurschmann Spiral100% (9)
- MRCPCH Clinical: Short Cases, History Taking & Communication Skills 3eDocument19 pagesMRCPCH Clinical: Short Cases, History Taking & Communication Skills 3ePasTestBooks100% (5)
- Karen - S Notes-Clinical ExaminationDocument11 pagesKaren - S Notes-Clinical ExaminationGanesh Namasivayam100% (3)
- Nbme 1 Block 1-4Document75 pagesNbme 1 Block 1-4Eimad Atif100% (1)
- Pediatric Triage PatDocument52 pagesPediatric Triage Patdrsapnataneja100% (1)
- Head To Toe Physical Assessment ChecklistDocument16 pagesHead To Toe Physical Assessment ChecklistMichael Allen Fadriquel100% (10)
- Step 1 Uworld PDFDocument25 pagesStep 1 Uworld PDFRegents Park Business Center100% (1)
- Pediatric EmergenciesDocument79 pagesPediatric Emergenciesأحمد سعد الديوه جيNo ratings yet
- Head To Toe Assessment in 5 MinutesDocument30 pagesHead To Toe Assessment in 5 Minutesdabyers8150No ratings yet
- Paediatric History and Examination 08092012-2Document10 pagesPaediatric History and Examination 08092012-2Shahin KazemzadehNo ratings yet
- Valvular Heart DiseaseDocument27 pagesValvular Heart DiseaseOwen J. WieseNo ratings yet
- Respiratory Video ScriptDocument3 pagesRespiratory Video ScriptNav KovNo ratings yet
- Initial Assessment and Secondary Survey GuideDocument14 pagesInitial Assessment and Secondary Survey GuideMelery LaraNo ratings yet
- Paed Examination Patient - Co.ukDocument9 pagesPaed Examination Patient - Co.ukraz2000No ratings yet
- Worksheet#1-Vital SignsDocument7 pagesWorksheet#1-Vital SignsCj MayoyoNo ratings yet
- Differential Diagnosis and Approach To A Heart Murmur in Term InfantsDocument10 pagesDifferential Diagnosis and Approach To A Heart Murmur in Term Infantsdeddy ekaNo ratings yet
- Pediatric Diagnosis PedDocument153 pagesPediatric Diagnosis PedIceNo ratings yet
- Lecture 1 ApgarDocument5 pagesLecture 1 Apgarapi-264459929No ratings yet
- 006 Assesment of Renal PatientDocument28 pages006 Assesment of Renal Patientbyrock66No ratings yet
- Assesment of The Newborn Baby-KuliahDocument66 pagesAssesment of The Newborn Baby-KuliahDhana AstikaNo ratings yet
- Assessing Preterm BabyDocument5 pagesAssessing Preterm BabyJoyce Kathreen Ebio LopezNo ratings yet
- Blood and Pulse Measaurment Topic 1Document17 pagesBlood and Pulse Measaurment Topic 1Amro AzrakNo ratings yet
- MRCPCH Clinical Short Cases History Taking Communication Skills 3e PDFDocument19 pagesMRCPCH Clinical Short Cases History Taking Communication Skills 3e PDFNirubhana Arunthavasothy100% (1)
- Care of The High Risk NewbornDocument309 pagesCare of The High Risk NewbornClaire Alvarez OngchuaNo ratings yet
- Assessing The Newborn and Infant-NewDocument11 pagesAssessing The Newborn and Infant-NewJan Jamison ZuluetaNo ratings yet
- Pals HandoutDocument49 pagesPals HandoutYasir AshfaqNo ratings yet
- The First Few HoursDocument8 pagesThe First Few HoursAili BellissimaNo ratings yet
- Nilai Normal Vital PediatriDocument4 pagesNilai Normal Vital PediatriEkaPutri AzizNo ratings yet
- Assesment of The Newborn Baby-KuliahDocument67 pagesAssesment of The Newborn Baby-Kuliahamel015No ratings yet
- Head To Toe Assessment in 5 Minutes or MoreDocument12 pagesHead To Toe Assessment in 5 Minutes or MoreTSPANNo ratings yet
- ToF ScriptDocument6 pagesToF ScriptCaity YoungNo ratings yet
- Pediatric Clinical ExaminationDocument37 pagesPediatric Clinical ExaminationHalema Al OkshNo ratings yet
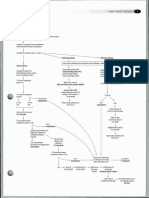
- 94 Heart Problems in Children: Gradient, Between The Left Ventricle and The Aorta. This Gradient Can Be MeaDocument1 page94 Heart Problems in Children: Gradient, Between The Left Ventricle and The Aorta. This Gradient Can Be MeaFernando VillavicencioNo ratings yet
- Pediatrics RemarksDocument62 pagesPediatrics RemarksGÖKSU SAYGILINo ratings yet
- High Risk New BornDocument5 pagesHigh Risk New BornAparna KinginiNo ratings yet
- Developmental MilestoneDocument11 pagesDevelopmental MilestoneGiselle EstoquiaNo ratings yet
- Paediatrics: Hannah Cooke, 2016/17Document99 pagesPaediatrics: Hannah Cooke, 2016/17james.a.blairNo ratings yet
- Assessment of NeonateDocument11 pagesAssessment of NeonateAbhishek GirdharNo ratings yet
- Ajal Hamza 403Document2 pagesAjal Hamza 403ajal hamzaNo ratings yet
- Mainit National High SchoolDocument4 pagesMainit National High Schoolfe delgadoNo ratings yet
- UntitledDocument59 pagesUntitledRobin KeaneNo ratings yet
- Assessment of Intrauterine Fetal Well BeingDocument11 pagesAssessment of Intrauterine Fetal Well Beingsagi mu100% (1)
- Growth and Development Milestones HESI HintsDocument12 pagesGrowth and Development Milestones HESI HintsJen Guthrie89% (9)
- Overview of Child HealthDocument81 pagesOverview of Child HealthSamer FarhanNo ratings yet
- Physical Examination in PaediatricsDocument162 pagesPhysical Examination in PaediatricsUsman Ali100% (1)
- Pendekatan Pada Pasien Anak (anamnesis+PF)Document25 pagesPendekatan Pada Pasien Anak (anamnesis+PF)Sarah AgustinNo ratings yet
- DiagnosisDocument5 pagesDiagnosisapi-300851869No ratings yet
- Atrial Septal DefectDocument5 pagesAtrial Septal DefectAnonymous MWd5UOUuiyNo ratings yet
- Mpilo Hospital Paeds Rescuscitation Manual-1Document38 pagesMpilo Hospital Paeds Rescuscitation Manual-1CFTCNo ratings yet
- Pediatric NotesDocument4 pagesPediatric NotesJincy PrinceNo ratings yet
- CVS ExamDocument35 pagesCVS Examtravis efraimNo ratings yet
- Physical Exam Guide for Pediatric SurgeonsDocument7 pagesPhysical Exam Guide for Pediatric SurgeonsMuhammadRifqiFarizanAkbarNo ratings yet
- 19 HTTP Familydoctor Org Familydoctor en Health Tools Search by Symptom Chest Pain Acute HTMLDocument5 pages19 HTTP Familydoctor Org Familydoctor en Health Tools Search by Symptom Chest Pain Acute HTMLYasaan ChaudharyNo ratings yet
- Procedure On Basic Life Support: General ConceptsDocument4 pagesProcedure On Basic Life Support: General Conceptsmalleshwari athramNo ratings yet
- Current Practice: ChildDocument3 pagesCurrent Practice: ChildRita ErmuracheNo ratings yet
- Pediatric Respiratory Emergencies: Nancy A. Johnson, Rrt/NpsDocument67 pagesPediatric Respiratory Emergencies: Nancy A. Johnson, Rrt/NpsAli Obadi AlhalemyNo ratings yet
- LWW BATES 03 Head To Toe Child Transcript FINALDocument12 pagesLWW BATES 03 Head To Toe Child Transcript FINALfrank garrettNo ratings yet
- Child HealthDocument12 pagesChild HealthHussain AliNo ratings yet
- The Asthma and Allergy Action Plan for Kids: A Complete Program to Help Your Child Live a Full and Active LifeFrom EverandThe Asthma and Allergy Action Plan for Kids: A Complete Program to Help Your Child Live a Full and Active LifeNo ratings yet
- The Australian Kids' Health Book: The Essential A-Z Guide to Emergencies , Baby Care and Common Childhood IllnessesFrom EverandThe Australian Kids' Health Book: The Essential A-Z Guide to Emergencies , Baby Care and Common Childhood IllnessesNo ratings yet
- Acid Reflux in Children: How Healthy Eating Can Fix Your Child's Asthma, Allergies, Obesity, Nasal Congestion, Cough & CroupFrom EverandAcid Reflux in Children: How Healthy Eating Can Fix Your Child's Asthma, Allergies, Obesity, Nasal Congestion, Cough & CroupNo ratings yet
- Choking, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandChoking, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Your Roadmap to Successful Asthma Treatment: A Parent's Guide to Preparing for Your Child's Doctor Visits and Long-Term CareFrom EverandYour Roadmap to Successful Asthma Treatment: A Parent's Guide to Preparing for Your Child's Doctor Visits and Long-Term CareNo ratings yet
- The Reye Syndrome Sourcebook: A Concise Guide for Parents and PatientsFrom EverandThe Reye Syndrome Sourcebook: A Concise Guide for Parents and PatientsNo ratings yet
- Cardio Exam Checklist2 PDFDocument1 pageCardio Exam Checklist2 PDFDawoodAslamNo ratings yet
- Pediatrics patient admission detailsDocument3 pagesPediatrics patient admission detailsabcNo ratings yet
- Pathoma Errata UpdatesDocument1 pagePathoma Errata UpdatesGrupi KatërtNo ratings yet
- Table of Parasited (Parasitology)Document9 pagesTable of Parasited (Parasitology)abcNo ratings yet
- Medical For StudentsDocument1 pageMedical For StudentsabcNo ratings yet
- Case Scenario 1 BSN II EDocument2 pagesCase Scenario 1 BSN II EJohn Michael TaylanNo ratings yet
- Option D (Postductal Coarctation of The Aorta) Is CorrectDocument50 pagesOption D (Postductal Coarctation of The Aorta) Is Correctanimebests9No ratings yet
- Teaching Internal Medicine Pearls On The WardsDocument212 pagesTeaching Internal Medicine Pearls On The WardsAnonymous ZeqcLl100% (10)
- Assessment of The Heart-Neck Vessels-Peripheral Vessels-PULSEDocument27 pagesAssessment of The Heart-Neck Vessels-Peripheral Vessels-PULSEJonah R. MeranoNo ratings yet
- High Yield Notes From UW Q BlocksDocument159 pagesHigh Yield Notes From UW Q BlocksKunal Sharma100% (5)
- Perloff 2012 Chapter PdaDocument28 pagesPerloff 2012 Chapter PdaMuhammad IrfanNo ratings yet
- Cardiovascular For The MRCP Paces Station 3Document13 pagesCardiovascular For The MRCP Paces Station 3Ismail H A100% (1)
- Self-Assessment ANSWERS (MCQ)Document15 pagesSelf-Assessment ANSWERS (MCQ)Maria OnofreiNo ratings yet
- Guide to Physical Assessment Exam SkillsDocument44 pagesGuide to Physical Assessment Exam SkillsBernice EbbiNo ratings yet
- Tiki Taka CK CardiologyDocument46 pagesTiki Taka CK CardiologyChristian Jara100% (2)
- Cardiovascular SystemDocument74 pagesCardiovascular Systemاسامة محمد السيد رمضانNo ratings yet
- Case Stenosis Aorta + RegurgitationDocument58 pagesCase Stenosis Aorta + RegurgitationRuth Faustine Jontah RayoNo ratings yet
- Deviriligo Notes 12Document99 pagesDeviriligo Notes 12A Fish100% (1)
- MurmursDocument5 pagesMurmursAlexander G. Álvarez RojasNo ratings yet
- Chapter 20 Heart and Neck VesselsDocument10 pagesChapter 20 Heart and Neck Vesselsannoja selvaNo ratings yet
- Practical Cardiac AuscultationDocument15 pagesPractical Cardiac AuscultationAugusto Rojas CarrionNo ratings yet
- Med MapsDocument117 pagesMed MapsDukeNo ratings yet
- Medicine LMRDocument24 pagesMedicine LMRadiNo ratings yet
- Physical Assessment of Preeclamptic PatientDocument3 pagesPhysical Assessment of Preeclamptic PatientAndreiNo ratings yet
- Pulmonic Valve DiseaseDocument22 pagesPulmonic Valve Diseasesarguss14No ratings yet
- Peds Shelf NotesDocument88 pagesPeds Shelf Notesskeebs23100% (8)
- Nursing Mnemonics: Everything Made EASY Part 2: MemoryDocument5 pagesNursing Mnemonics: Everything Made EASY Part 2: MemoryCrystal Ann Monsale TadiamonNo ratings yet
- Common MurmurDocument2 pagesCommon MurmurKyWoNo ratings yet
- Bawasig Pediatric ExamDocument20 pagesBawasig Pediatric Examخلدون سليمNo ratings yet
- Mitral Stenosis and Regurgitation: Etiology, Symptoms, Exam, and ManagementDocument85 pagesMitral Stenosis and Regurgitation: Etiology, Symptoms, Exam, and ManagementWilliam Lie100% (2)