You might also like
- The Maximally Efficient and Optimally Effective Emergency Department: One Good Thing A DayFrom EverandThe Maximally Efficient and Optimally Effective Emergency Department: One Good Thing A DayNo ratings yet
- 1 s2.0 S2214139120301165 MainDocument6 pages1 s2.0 S2214139120301165 MainsarvitaNo ratings yet
- International Emergency Nursing: P. Roivainen, M.J. Hoikka, T.I. Ala-Kokko, M. K A Ari AinenDocument7 pagesInternational Emergency Nursing: P. Roivainen, M.J. Hoikka, T.I. Ala-Kokko, M. K A Ari AinenAinulNo ratings yet
- Managing Patient Expectations at Emergency Department Triage PDFDocument15 pagesManaging Patient Expectations at Emergency Department Triage PDFCaesar CeblonkNo ratings yet
- ADocument6 pagesAsinnanancyNo ratings yet
- Patient Satisfaction Reporting - A Cohort Study Comparing Reporting of Patient Satisfaction Pre-And Post-Discharge From HospitalDocument7 pagesPatient Satisfaction Reporting - A Cohort Study Comparing Reporting of Patient Satisfaction Pre-And Post-Discharge From HospitalnrlNo ratings yet
- The Impact of Nurse Rounding On Patient Satisfaction in A Medical-Surgical Hospital UnitDocument7 pagesThe Impact of Nurse Rounding On Patient Satisfaction in A Medical-Surgical Hospital UnitBheru LalNo ratings yet
- Evaluation of The Satisfaction Level of Patients Visiting Dental Emergency ServicesDocument4 pagesEvaluation of The Satisfaction Level of Patients Visiting Dental Emergency ServicesnatalyaNo ratings yet
- 43 JMSCRDocument9 pages43 JMSCRRajni KumariNo ratings yet
- Teamwork, Psychological Safety, and Patient SafetyDocument5 pagesTeamwork, Psychological Safety, and Patient SafetyMutiara100% (1)
- IranDocument5 pagesIranSandra RNo ratings yet
- Safe Surgery JournalDocument10 pagesSafe Surgery JournalNur LaelaNo ratings yet
- Evaluation of An Advanced Practice Provider Emergency Department Critical Care Step-Down UnitDocument11 pagesEvaluation of An Advanced Practice Provider Emergency Department Critical Care Step-Down UnitMiva MaviniNo ratings yet
- A Study On Waiting Time of The OPD Patient in A Multispecialty HospitalDocument6 pagesA Study On Waiting Time of The OPD Patient in A Multispecialty HospitalIJRASETPublicationsNo ratings yet
- The Effects of HealthService Delivery On Patient SatisfactionDocument5 pagesThe Effects of HealthService Delivery On Patient SatisfactiongudataaNo ratings yet
- Nursing Rounds: A Quality Improvement Project To Improve Outpatient SatisfactionDocument9 pagesNursing Rounds: A Quality Improvement Project To Improve Outpatient Satisfactionlina febriantiNo ratings yet
- Nursing Rounds: A Quality Improvement Project To Improve Outpatient SatisfactionDocument9 pagesNursing Rounds: A Quality Improvement Project To Improve Outpatient SatisfactionIkhsanNo ratings yet
- Er ReadingsDocument6 pagesEr ReadingsReginald UyNo ratings yet
- Patients' Waiting Time: Indices For Measuring Hospital EffectivenessDocument18 pagesPatients' Waiting Time: Indices For Measuring Hospital Effectivenessmr kevinNo ratings yet
- Intisari Permenkes No11 Tahun 2017Document8 pagesIntisari Permenkes No11 Tahun 2017Hari Putra PetirNo ratings yet
- 1136 4024 1 PBDocument7 pages1136 4024 1 PBTanish gogwalNo ratings yet
- Jurnal InternasionalDocument7 pagesJurnal InternasionalDina AryaniNo ratings yet
- Determinant of Nurses' Response Time in Emergency Department When Taking Care of A PatientDocument9 pagesDeterminant of Nurses' Response Time in Emergency Department When Taking Care of A PatientRuly AryaNo ratings yet
- 14186-Article Text-26331-5-10-20190611Document9 pages14186-Article Text-26331-5-10-20190611Al FatihNo ratings yet
- Format Review Article Title Article: Nama Mahasiswa: Muhammad Satya Arrif Zulhani NIM: 20171030029 URL Section PurposeDocument4 pagesFormat Review Article Title Article: Nama Mahasiswa: Muhammad Satya Arrif Zulhani NIM: 20171030029 URL Section PurposeMuhammad Satya EnzoNo ratings yet
- Patient Satisfaction As A Possible Indicator of Quality Surgical CareDocument6 pagesPatient Satisfaction As A Possible Indicator of Quality Surgical CarePutri Sholih Dewi IrdiantiNo ratings yet
- Asian Nursing ResearchDocument7 pagesAsian Nursing ResearchWayan Dyego SatyawanNo ratings yet
- Factors Affecting Patient's Satisfaction in Outpatient Clinics in Jordan: Cross-Sectional StudyDocument6 pagesFactors Affecting Patient's Satisfaction in Outpatient Clinics in Jordan: Cross-Sectional StudyAzzalfaAftaniNo ratings yet
- Patient Satisfaction Survey at Al-Nafees Hospital OPDDocument6 pagesPatient Satisfaction Survey at Al-Nafees Hospital OPDapouakone apouakoneNo ratings yet
- WJCCM: Critical Care MedicineDocument7 pagesWJCCM: Critical Care MedicineRodrigoSachiFreitasNo ratings yet
- Samikshya .EditedDocument8 pagesSamikshya .EditedSaru NiraulaNo ratings yet
- 10 1093@intqhc@mzx017 PDFDocument6 pages10 1093@intqhc@mzx017 PDFMeli SariNo ratings yet
- Jurnal Kesehatan Masyarakat: Caring Environment Model in Emergency Services of Hospitals by Banyumas Public PerceptionDocument8 pagesJurnal Kesehatan Masyarakat: Caring Environment Model in Emergency Services of Hospitals by Banyumas Public PerceptionRiska KurniawatiNo ratings yet
- Effects of Nursing Rounds: On Patients' Call Light Use, Satisfaction, and SafetyDocument13 pagesEffects of Nursing Rounds: On Patients' Call Light Use, Satisfaction, and SafetyhanimozaghiNo ratings yet
- 1 Paper EmergencyDepartmentPatientProcessFlowDocument6 pages1 Paper EmergencyDepartmentPatientProcessFlowYey PahmateeNo ratings yet
- The Relationship Between Waiting Time and Patient Satisfaction in The Outpatient of Public Hospital in BanjarbaruDocument7 pagesThe Relationship Between Waiting Time and Patient Satisfaction in The Outpatient of Public Hospital in BanjarbaruWijayadi SuyonoNo ratings yet
- The Effect of Structured Nursing Rounds On The Level Nursing Care Satisfaction of Patient in A Selected Tertiary Care Hospital, PuducherryDocument15 pagesThe Effect of Structured Nursing Rounds On The Level Nursing Care Satisfaction of Patient in A Selected Tertiary Care Hospital, PuducherryIJAR JOURNALNo ratings yet
- Patient Satisfaction Survey at A Tertiary Care Speciality HospitalDocument5 pagesPatient Satisfaction Survey at A Tertiary Care Speciality HospitalJasneep0% (1)
- Improving The Patient's Experience in The Emergency Department During COVID-19 Pandemic A Community-Based Analysis From Western Saudi Arabia.Document5 pagesImproving The Patient's Experience in The Emergency Department During COVID-19 Pandemic A Community-Based Analysis From Western Saudi Arabia.editorial.boardNo ratings yet
- Assessment of Clients' Satisfaction With Health Service Deliveries at Jimma University Specialized HospitalDocument10 pagesAssessment of Clients' Satisfaction With Health Service Deliveries at Jimma University Specialized HospitalUrfan MajidNo ratings yet
- Improving Team Structure and Communication: EffectiveDocument31 pagesImproving Team Structure and Communication: EffectiveSutisna NisaNo ratings yet
- ICU vs. Ward PU PreventionDocument59 pagesICU vs. Ward PU PreventionrantiNo ratings yet
- CEA UnlockedDocument12 pagesCEA UnlockedK. O.No ratings yet
- The Effect of An Emergency Department Dedicated Midtrack Area On Patient FlowDocument6 pagesThe Effect of An Emergency Department Dedicated Midtrack Area On Patient FlowBeny HermawanNo ratings yet
- 17 ManarDocument14 pages17 Manarheba abd elazizNo ratings yet
- The Influence of A Service Instrument For Measuring Patient Satisfaction in Multispecialty Teaching Hospital at OdishaDocument9 pagesThe Influence of A Service Instrument For Measuring Patient Satisfaction in Multispecialty Teaching Hospital at OdishaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Effectiveness of Psychoeducational Program On Psychological Outcomes Among Patients Undergoing Cardiac Surgery in Khartoum2017 639Document5 pagesEffectiveness of Psychoeducational Program On Psychological Outcomes Among Patients Undergoing Cardiac Surgery in Khartoum2017 639Ishraga AlbashierNo ratings yet
- International Emergency Nursing: SciencedirectDocument7 pagesInternational Emergency Nursing: SciencedirectKavin Zank JuniorNo ratings yet
- Patient's Satisfaction With Nursing Care Provided in Selected Areas of Tertiary Care Hospital 1Document13 pagesPatient's Satisfaction With Nursing Care Provided in Selected Areas of Tertiary Care Hospital 1Anonymous CuWlCKxXkENo ratings yet
- Emergency Department Patient Satisfaction AssessmeDocument6 pagesEmergency Department Patient Satisfaction AssessmeJeniffer PeñarandaNo ratings yet
- 1 Paper EmergencyDepartmentPatientProcessFlowDocument6 pages1 Paper EmergencyDepartmentPatientProcessFlowandika fahruroziNo ratings yet
- Hiper 5Document8 pagesHiper 5dezunNo ratings yet
- Exploring Patient Safety Culture in Emergency DepartmentsDocument7 pagesExploring Patient Safety Culture in Emergency Departmentsmuhammad ismailNo ratings yet
- Effects of Nursing RoundsDocument14 pagesEffects of Nursing RoundsTatiana SiregarNo ratings yet
- TJEM - Factors Affecting The Accuracy of Nurse Triage in Tertiary Care E.RDocument5 pagesTJEM - Factors Affecting The Accuracy of Nurse Triage in Tertiary Care E.RIntanPermataSyariNo ratings yet
- Summer Training Project Report On Patient Satisfaction Regarding Health CareDocument13 pagesSummer Training Project Report On Patient Satisfaction Regarding Health Care089 satyamNo ratings yet
- Relationship Between Nurse Case Manager's Communication Skills and Patient Satisfaction at Hospital in JakartaDocument6 pagesRelationship Between Nurse Case Manager's Communication Skills and Patient Satisfaction at Hospital in Jakartakritis ardiansyahNo ratings yet
- Shortstay LiteratureDocument5 pagesShortstay LiteratureDon RicaforteNo ratings yet
- International Journal of Nursing Sciences: Jung Hee Kim, Jung Lim Lee, Eun Man KimDocument7 pagesInternational Journal of Nursing Sciences: Jung Hee Kim, Jung Lim Lee, Eun Man KimAnna FadhilaNo ratings yet
- 857 1857 1 PBDocument4 pages857 1857 1 PBJesselle LasernaNo ratings yet
- NCSBN's Reviews For The NCLEX-RN & Nclex-PN: Weekly Study PlanDocument3 pagesNCSBN's Reviews For The NCLEX-RN & Nclex-PN: Weekly Study PlanJesselle LasernaNo ratings yet
- Pathophysiology of PneumoniaDocument2 pagesPathophysiology of PneumoniaJesselle LasernaNo ratings yet
- CE Mild Traumatic Brain Injury.24Document7 pagesCE Mild Traumatic Brain Injury.24Jesselle LasernaNo ratings yet
- European Down Syndrome Association: February 2016Document7 pagesEuropean Down Syndrome Association: February 2016Jesselle LasernaNo ratings yet
- Problem ListDocument1 pageProblem ListJesselle LasernaNo ratings yet
- Metronidazole Ds Case Pre 4th YrDocument2 pagesMetronidazole Ds Case Pre 4th YrJesselle LasernaNo ratings yet
- Basic Concepts On Communityacquired Bacterial Pneumonia in PediatricsDocument6 pagesBasic Concepts On Communityacquired Bacterial Pneumonia in PediatricsJesselle LasernaNo ratings yet
- Unasyn Drug GuideDocument2 pagesUnasyn Drug GuideJesselle LasernaNo ratings yet
- Care of Patient With Copd: Chronic Obstructive Pulmonary DiseaseDocument32 pagesCare of Patient With Copd: Chronic Obstructive Pulmonary DiseaseJesselle LasernaNo ratings yet
- 188-Knowledge, Attitude and Practice On Antenatal CareDocument9 pages188-Knowledge, Attitude and Practice On Antenatal CareJesselle LasernaNo ratings yet
- Wvsu Scholarship f09Document2 pagesWvsu Scholarship f09Jesselle LasernaNo ratings yet
- Down Syndrome (DS) and Hirschsprung's Disease (HSCR)Document3 pagesDown Syndrome (DS) and Hirschsprung's Disease (HSCR)Jesselle LasernaNo ratings yet
- 222 765 1 PBDocument8 pages222 765 1 PBJesselle LasernaNo ratings yet
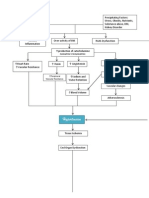
- PathoPhysiology of Hypertension DiagramDocument4 pagesPathoPhysiology of Hypertension DiagramKat Taasin100% (1)
- NCP CVA Activity IntoleranceDocument2 pagesNCP CVA Activity IntoleranceJesselle LasernaNo ratings yet
- Nursing Diagnoses & Interventions for Schizophrenia ClientDocument6 pagesNursing Diagnoses & Interventions for Schizophrenia ClientJesselle LasernaNo ratings yet
- Schematic Diagram of Pleural EffusionDocument2 pagesSchematic Diagram of Pleural EffusionJesselle Laserna0% (1)
- ReadmeDocument2 pagesReadmeJesselle LasernaNo ratings yet
- Barthel Index (0-20)Document2 pagesBarthel Index (0-20)Yessika Adelwin Natalia95% (19)
- Review of Systems Cheat SheetDocument2 pagesReview of Systems Cheat Sheetarmymedic7No ratings yet
- BoneDocument5 pagesBoneJesselle LasernaNo ratings yet
- Healthcare Financing in IndiADocument86 pagesHealthcare Financing in IndiAGeet Sheil67% (3)
- Cut Sheet GE Infinia HawkeyeDocument2 pagesCut Sheet GE Infinia HawkeyeselvamejiaNo ratings yet
- Bu SuryaniDocument68 pagesBu SuryaniMaulana SaputraNo ratings yet
- Drug StudyDocument17 pagesDrug StudyJoan RabeNo ratings yet
- Case StudyDocument5 pagesCase StudyHomework PingNo ratings yet
- Ross University 2010-2011 Pre-Residency Planning GuideDocument61 pagesRoss University 2010-2011 Pre-Residency Planning GuidescatteredbrainNo ratings yet
- ESB 2018 Abstract Proceedings 4Document1,099 pagesESB 2018 Abstract Proceedings 4Alan PolancoNo ratings yet
- Cebu Normal University College of NursingDocument7 pagesCebu Normal University College of NursingGwyn RosalesNo ratings yet
- Referat Arlha PemDocument65 pagesReferat Arlha PemDicky Delonge LesmanaNo ratings yet
- EMQ and SAQ Revision QuestionsDocument12 pagesEMQ and SAQ Revision QuestionsSanathRaoNo ratings yet
- Hospitals Penalized for Refusing Emergency CareDocument6 pagesHospitals Penalized for Refusing Emergency CareApril Isidro100% (1)
- Ohi 2Document6 pagesOhi 2api-242024640No ratings yet
- Hospital Report PDFDocument28 pagesHospital Report PDFGaurav Chaudhary Alig100% (1)
- Compartment SyndromeDocument29 pagesCompartment SyndromeFazmial UjirNo ratings yet
- Montelukast SodiumDocument10 pagesMontelukast SodiumikhasilNo ratings yet
- Malaysia - Kontrak - Pusat - Ubat-Ubatan - KKM - 20.03.12Document21 pagesMalaysia - Kontrak - Pusat - Ubat-Ubatan - KKM - 20.03.12Anuj Mairh0% (1)
- Prevalence of thyroid dysfunctionDocument32 pagesPrevalence of thyroid dysfunctiondalip kumarNo ratings yet
- IM Shelf - AmbossDocument61 pagesIM Shelf - AmbossHaadi AliNo ratings yet
- R - MN R - 1 Z: Mkg-Xixltechlib/1 T/06Document48 pagesR - MN R - 1 Z: Mkg-Xixltechlib/1 T/06Jhantu MazumderNo ratings yet
- Calculation SeatworkDocument2 pagesCalculation SeatworkBenedict James BermasNo ratings yet
- CPM14th DIABETES Food GuideDocument21 pagesCPM14th DIABETES Food GuideXhiariwen Bayro0% (1)
- Bowel Preparation Colon ResectionDocument28 pagesBowel Preparation Colon ResectioncristiangallardovNo ratings yet
- Drug Study DengueDocument3 pagesDrug Study DengueiamELHIZANo ratings yet
- CBTDocument21 pagesCBTsavvy_as_98No ratings yet
- NCP Infection NewDocument3 pagesNCP Infection NewXerxes DejitoNo ratings yet
- Elderly Care IndiaDocument3 pagesElderly Care IndiakasurvarNo ratings yet
- Denumire Comerciala DCI Forma Farmaceutica ConcentratieDocument4 pagesDenumire Comerciala DCI Forma Farmaceutica ConcentratieAlina CiugureanuNo ratings yet
- Transcultural NursingDocument13 pagesTranscultural NursingHassen ZabalaNo ratings yet
- Notice: Agency Information Collection Activities Proposals, Submissions, and ApprovalsDocument2 pagesNotice: Agency Information Collection Activities Proposals, Submissions, and ApprovalsJustia.comNo ratings yet
- BLEEDING TIME AND CLOTTING TIME TESTSDocument30 pagesBLEEDING TIME AND CLOTTING TIME TESTScharutha gopalNo ratings yet