You might also like
- Efficiency of Care and Satisfaction For Head Injury Patients at Emergency Department in Mansoura Emergency HospitalDocument11 pagesEfficiency of Care and Satisfaction For Head Injury Patients at Emergency Department in Mansoura Emergency HospitalJesselle LasernaNo ratings yet
- Wvsu Scholarship f09Document2 pagesWvsu Scholarship f09Jesselle LasernaNo ratings yet
- NCSBN's Reviews For The NCLEX-RN & Nclex-PN: Weekly Study PlanDocument3 pagesNCSBN's Reviews For The NCLEX-RN & Nclex-PN: Weekly Study PlanJesselle LasernaNo ratings yet
- Pathophysiology of PneumoniaDocument2 pagesPathophysiology of PneumoniaJesselle LasernaNo ratings yet
- 222 765 1 PBDocument8 pages222 765 1 PBJesselle LasernaNo ratings yet
- Problem ListDocument1 pageProblem ListJesselle LasernaNo ratings yet
- 857 1857 1 PBDocument4 pages857 1857 1 PBJesselle LasernaNo ratings yet
- European Down Syndrome Association: February 2016Document7 pagesEuropean Down Syndrome Association: February 2016Jesselle LasernaNo ratings yet
- Basic Concepts On Communityacquired Bacterial Pneumonia in PediatricsDocument6 pagesBasic Concepts On Communityacquired Bacterial Pneumonia in PediatricsJesselle LasernaNo ratings yet
- 188-Knowledge, Attitude and Practice On Antenatal CareDocument9 pages188-Knowledge, Attitude and Practice On Antenatal CareJesselle LasernaNo ratings yet
- Metronidazole Ds Case Pre 4th YrDocument2 pagesMetronidazole Ds Case Pre 4th YrJesselle LasernaNo ratings yet
- NCP CVA Activity IntoleranceDocument2 pagesNCP CVA Activity IntoleranceJesselle LasernaNo ratings yet
- Unasyn Drug GuideDocument2 pagesUnasyn Drug GuideJesselle LasernaNo ratings yet
- Down Syndrome (DS) and Hirschsprung's Disease (HSCR)Document3 pagesDown Syndrome (DS) and Hirschsprung's Disease (HSCR)Jesselle LasernaNo ratings yet
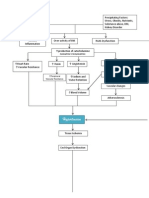
- PathoPhysiology of Hypertension DiagramDocument4 pagesPathoPhysiology of Hypertension DiagramKat Taasin100% (1)
- Care of Patient With Copd: Chronic Obstructive Pulmonary DiseaseDocument32 pagesCare of Patient With Copd: Chronic Obstructive Pulmonary DiseaseJesselle LasernaNo ratings yet
- Barthel Index (0-20)Document2 pagesBarthel Index (0-20)Yessika Adelwin Natalia95% (19)
- ReadmeDocument2 pagesReadmeJesselle LasernaNo ratings yet
- Review of Systems Cheat SheetDocument2 pagesReview of Systems Cheat Sheetarmymedic7No ratings yet
- BoneDocument5 pagesBoneJesselle LasernaNo ratings yet
- Nursing Diagnoses & Interventions for Schizophrenia ClientDocument6 pagesNursing Diagnoses & Interventions for Schizophrenia ClientJesselle LasernaNo ratings yet
- Schematic Diagram of Pleural EffusionDocument2 pagesSchematic Diagram of Pleural EffusionJesselle Laserna0% (1)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- SPO102 - Sports MarketingDocument8 pagesSPO102 - Sports MarketingpakizaNo ratings yet
- Cognitive Conditioning Program: Cairns Sports Performance Clinic & PNG High PerformanceDocument8 pagesCognitive Conditioning Program: Cairns Sports Performance Clinic & PNG High PerformanceBogdan GheorghiuNo ratings yet
- Assessment of Concussion from Sideline to ClinicDocument36 pagesAssessment of Concussion from Sideline to ClinicCiiFitriNo ratings yet
- Concussion Management PlanDocument4 pagesConcussion Management Planapi-310029510No ratings yet
- 2023 USATKD Kyorugi Rules - Modified Head ContactDocument12 pages2023 USATKD Kyorugi Rules - Modified Head Contactyoussef mebarekNo ratings yet
- Acute Concussion Evaluation Care Plan - SchoolDocument2 pagesAcute Concussion Evaluation Care Plan - SchoolANo ratings yet
- Traumatic Brain InjuryDocument15 pagesTraumatic Brain InjuryAbbey Janine Mandapat Passi100% (3)
- Scope 020115 DebateDocument3 pagesScope 020115 Debateapi-354947086No ratings yet
- The Colleges of Medicine of South AfricaDocument4 pagesThe Colleges of Medicine of South AfricaRichard100% (1)
- Medico Legal Aspects of Physical InjuriesDocument111 pagesMedico Legal Aspects of Physical InjuriesRainnie McBeeNo ratings yet
- Head Injury - HandoutDocument10 pagesHead Injury - HandoutMohd Hisyamuddin SaharudinNo ratings yet
- Sarah CroftDocument11 pagesSarah CroftTARUNNo ratings yet
- 2016 - Are There Subconcussive Neuropsychological Effects in Youth Sports? An Exploratory Study of High - and Low-Contact SportsDocument8 pages2016 - Are There Subconcussive Neuropsychological Effects in Youth Sports? An Exploratory Study of High - and Low-Contact SportsRaúl VerdugoNo ratings yet
- Instant Download Ebook PDF Essentials of Athletic Injury Management 10th Edition PDF ScribdDocument41 pagesInstant Download Ebook PDF Essentials of Athletic Injury Management 10th Edition PDF Scribdjune.thompson131100% (40)
- The Rain: Phase 1Document113 pagesThe Rain: Phase 1William ArnoldNo ratings yet
- CNS Vital Signs Interpretation Guide: Business OfficeDocument15 pagesCNS Vital Signs Interpretation Guide: Business OfficeJason WeaverNo ratings yet
- SCAT3Document5 pagesSCAT3DanielleNo ratings yet
- Case Study of Head Injury SijiDocument30 pagesCase Study of Head Injury SijiJinal PatelNo ratings yet
- Rey Auditory Verbal Learning Test NOC LinkDocument3 pagesRey Auditory Verbal Learning Test NOC LinkAmandavictooria67% (3)
- Concussion Prevention and TreatmentDocument6 pagesConcussion Prevention and Treatmentapi-394390742No ratings yet
- TCE PhysiotherapyDocument73 pagesTCE PhysiotherapyCarolina IzquierdoNo ratings yet
- Capstone Lit Review Fall 2017Document16 pagesCapstone Lit Review Fall 2017api-383946209No ratings yet
- EAPP Quarter 01 Modules CNo Answer KeyDocument185 pagesEAPP Quarter 01 Modules CNo Answer KeyKasey Buenviaje100% (3)
- Passages Part 3Document27 pagesPassages Part 3Insignia D.No ratings yet
- Julius Whittier LawsuitDocument22 pagesJulius Whittier LawsuitHouston ChronicleNo ratings yet
- Activity in EAPPDocument3 pagesActivity in EAPPElijah AquinoNo ratings yet
- Albuquerque Public Schools: Athletic and Activity Code of ConductDocument7 pagesAlbuquerque Public Schools: Athletic and Activity Code of Conductstephie4No ratings yet
- Scat 5Document9 pagesScat 5api-347625375No ratings yet
- 10 Good Abstract Examples That Will Kickstart Your BrainDocument11 pages10 Good Abstract Examples That Will Kickstart Your BrainAlbieJane CatotoNo ratings yet
- First Aid On TaekwondoDocument5 pagesFirst Aid On TaekwondoJoshua De Leon TuasonNo ratings yet