You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Kidambi and Aakella 2007 (Social Audits in Andhra)Document2 pagesKidambi and Aakella 2007 (Social Audits in Andhra)rozgarNo ratings yet
- Speakers & Workshop Leaders: Catherine DayDocument4 pagesSpeakers & Workshop Leaders: Catherine DaylilikaliaNo ratings yet
- Shut-Up WriteDocument21 pagesShut-Up Writeapi-253744436No ratings yet
- Prelim Facilitating AnswerDocument2 pagesPrelim Facilitating AnswerSarah Imarah Mislang100% (2)
- Use Mathematical Concept and TechniquesDocument67 pagesUse Mathematical Concept and Techniquesvillamor niez63% (8)
- Lesson Plan ReadingDocument7 pagesLesson Plan ReadingNiar SamandiNo ratings yet
- A Case Study On The Implementation of Knowledge ManagementDocument10 pagesA Case Study On The Implementation of Knowledge ManagementEmmangeorgeNo ratings yet
- Tera NeterDocument4 pagesTera NeterNabil Roufail100% (3)
- AngajawiDocument13 pagesAngajawiAhmad BasoNo ratings yet
- Lecture On ProphethoodDocument31 pagesLecture On ProphethoodDanish Uttra100% (1)
- Centrifugal ForceDocument5 pagesCentrifugal Forceasd3e23No ratings yet
- Educational Communication For DevelopmenDocument34 pagesEducational Communication For DevelopmenBryan GH VargasNo ratings yet
- Isi 2Document15 pagesIsi 2Nasser KalanNo ratings yet
- Four Days Late, But Still On TimeDocument5 pagesFour Days Late, But Still On TimeK Songput100% (1)
- The ShawlDocument3 pagesThe Shawlapi-299585557No ratings yet
- Vasthu Part1Document147 pagesVasthu Part1vinay100% (1)
- Vykhanasaagma 1Document10 pagesVykhanasaagma 1Sai Ranganath BNo ratings yet
- A Comparative Study Between Introverts and Extraverts in Their Conforming Behaviours Among Students at Galaxy International School in GhanaDocument4 pagesA Comparative Study Between Introverts and Extraverts in Their Conforming Behaviours Among Students at Galaxy International School in Ghanadecker4449No ratings yet
- Listening To Australia - IntermediateDocument82 pagesListening To Australia - IntermediateAnonymous RYbWvk83% (6)
- MS HandoutDocument3 pagesMS HandoutJayant JawanjalNo ratings yet
- Binder 1996 FluencyDocument35 pagesBinder 1996 FluencyAnonymous YfCPPhri8lNo ratings yet
- First A Poem Must Be MagicalDocument11 pagesFirst A Poem Must Be MagicalBERNARDITA E. GUTIB100% (1)
- The Tao of Pooh - SummaryDocument3 pagesThe Tao of Pooh - Summaryjak-as100% (1)
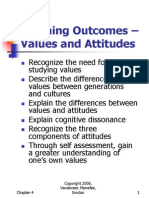
- Learning Outcomes - Values and Attitudes: Vandeveer, Menefee, Sinclair 1Document22 pagesLearning Outcomes - Values and Attitudes: Vandeveer, Menefee, Sinclair 1Nurhikmah RnNo ratings yet
- RVR JC College of Engineering Question Bank 1Document2 pagesRVR JC College of Engineering Question Bank 1MOHAMMED AFZALNo ratings yet
- CAMEO Manual 1 1b3Document198 pagesCAMEO Manual 1 1b3Bogdan TautNo ratings yet
- Paul Éluard (1895-1952) : Life: Les Yeux Fertiles (1936) - L'Immaculée Conception (1930)Document5 pagesPaul Éluard (1895-1952) : Life: Les Yeux Fertiles (1936) - L'Immaculée Conception (1930)api-357156106100% (1)
- Daily Lesson PlanDocument2 pagesDaily Lesson PlanDivine OngNo ratings yet
- Leonardo DavinciDocument12 pagesLeonardo DavinciBry CunalNo ratings yet
- Advice To Graduate School Recommendation Letter WritersDocument8 pagesAdvice To Graduate School Recommendation Letter WritersVishal GuptaNo ratings yet