You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Tonsillectomy Slides 050427Document62 pagesTonsillectomy Slides 050427Aidiel FikriNo ratings yet
- DRUG STUDY EpinephrineDocument2 pagesDRUG STUDY EpinephrineCarlo Francisco D. Canto78% (9)
- RN Viray ResumefinalDocument1 pageRN Viray Resumefinalapi-661315652No ratings yet
- NeocortexDocument1 pageNeocortexZeromalisNilNo ratings yet
- Aiswarya Krishna: Professional SummaryDocument4 pagesAiswarya Krishna: Professional SummaryRejoy RadhakrishnanNo ratings yet
- Nutrition and Fluid ManagementDocument1 pageNutrition and Fluid ManagementCeci NiheNo ratings yet
- Arterial Blood GasesDocument9 pagesArterial Blood GasesJohn BattleNo ratings yet
- MediShield Life: Better Protection for AllDocument20 pagesMediShield Life: Better Protection for Alljakovach7No ratings yet
- International Patient Safety Goals IPSGDocument20 pagesInternational Patient Safety Goals IPSGShafique HussainNo ratings yet
- Advanced Level - ReadingDocument5 pagesAdvanced Level - ReadingLarry SmithNo ratings yet
- Hepatic EncephalopathyDocument16 pagesHepatic Encephalopathyjh_ajjNo ratings yet
- Renr Study GuideDocument57 pagesRenr Study GuideJerilee SoCute Watts92% (12)
- Cons Study Summary QuiestionsDocument124 pagesCons Study Summary QuiestionsCons Miyu HimeNo ratings yet
- Oxy CadDocument21 pagesOxy CadrlinaoNo ratings yet
- Preceptorship Journal 2Document3 pagesPreceptorship Journal 2api-325099570No ratings yet
- Lab Technician or Clerical or BankingDocument2 pagesLab Technician or Clerical or Bankingapi-76931734No ratings yet
- Abdominal Pain DischargeDocument2 pagesAbdominal Pain Dischargemfa40No ratings yet
- Megan Talbott ResumeDocument3 pagesMegan Talbott Resumeapi-291314145No ratings yet
- Haematology Laboratory User Handbook - Updated July 2020 JWDocument25 pagesHaematology Laboratory User Handbook - Updated July 2020 JWBassam AlharaziNo ratings yet
- TDM Request Form Provides Drug MonitoringDocument3 pagesTDM Request Form Provides Drug MonitoringWildan Setyo RayandiNo ratings yet
- Shock Power PointDocument24 pagesShock Power PointmarwaNo ratings yet
- Cardiac biomarkers: cTnI and NT-proBNPDocument5 pagesCardiac biomarkers: cTnI and NT-proBNPAntonio SessaNo ratings yet
- Alteration of ConsciousnessDocument71 pagesAlteration of Consciousnessmarauder_popNo ratings yet
- Tongue in Complete DentureDocument8 pagesTongue in Complete DentureAman SachdevaNo ratings yet
- RENR Review Utech 8Document34 pagesRENR Review Utech 8natalieshirley100% (3)
- Chapter 18 Personality DisordersDocument10 pagesChapter 18 Personality DisordersCatia Fernandes100% (2)
- ORTHOPAEDICS TRAUMADocument33 pagesORTHOPAEDICS TRAUMARhomizal MazaliNo ratings yet
- CHRONIC RHINOSINUSTIS PRESENTATION, DIAGNOSIS AND MANAGEMENTDocument36 pagesCHRONIC RHINOSINUSTIS PRESENTATION, DIAGNOSIS AND MANAGEMENTAritro BhattacharjiNo ratings yet
- Nursing Notes Templates (Guidelines To Take Nursing Notes)Document20 pagesNursing Notes Templates (Guidelines To Take Nursing Notes)Rose100% (1)
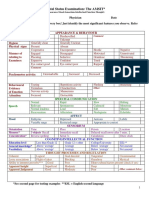
- Mental Status Examination: The AMSIT : Neat and Tidy DisshevelledDocument2 pagesMental Status Examination: The AMSIT : Neat and Tidy Disshevellednisreen100% (1)