You might also like
- Fractures of The Upper LimbDocument20 pagesFractures of The Upper LimbWendy Francisca Borquez PerezNo ratings yet
- Hip Neck Fracture, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHip Neck Fracture, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Malunion Delayed Union and Nonunion FracturesDocument31 pagesMalunion Delayed Union and Nonunion FracturesRasjad ChairuddinNo ratings yet
- Orthopedic examination techniques and common conditionsDocument226 pagesOrthopedic examination techniques and common conditionsMandisa Ndlovu Tenego0% (1)
- By DR - Mohammad Z. Abu Sheikha@: +pigmented Stones (Black Stone - Non Infected) (Brown Stone - Infected)Document11 pagesBy DR - Mohammad Z. Abu Sheikha@: +pigmented Stones (Black Stone - Non Infected) (Brown Stone - Infected)Nisreen Al-shareNo ratings yet
- Meningeal SyndromeDocument2 pagesMeningeal SyndromeEmi ValcovNo ratings yet
- Peripheral Nerve InjuriesDocument23 pagesPeripheral Nerve InjuriesUmar AzlanNo ratings yet
- Normal Pressure HydrocephalusDocument59 pagesNormal Pressure Hydrocephalusrys239No ratings yet
- Emtiaz Guide in SurgeryDocument25 pagesEmtiaz Guide in SurgeryMohamed AwadNo ratings yet
- ParaplegiaDocument7 pagesParaplegiaRigaga GopiNo ratings yet
- Fractures of Arm Forearm PDFDocument3 pagesFractures of Arm Forearm PDFjimNo ratings yet
- Spinal Cord TumorsDocument23 pagesSpinal Cord TumorsTahleel AltafNo ratings yet
- Gastroenterology: Diseases of The EsophagusDocument18 pagesGastroenterology: Diseases of The EsophagusKayeshiana30No ratings yet
- Combined Okell NotesDocument202 pagesCombined Okell Notessameeramw100% (5)
- Avascular NecrosisDocument3 pagesAvascular Necrosisahmad shaltoutNo ratings yet
- High Yield General Surgery Topics PDFDocument85 pagesHigh Yield General Surgery Topics PDF1031 Muhammad zaryabNo ratings yet
- Undergraduate Neurosurgery Lecture NotesDocument124 pagesUndergraduate Neurosurgery Lecture NotesLuquiitas LasernaNo ratings yet
- Orthopedics Notes NeetpgDocument4 pagesOrthopedics Notes NeetpgGIST (Gujarat Institute of Science & Technology)No ratings yet
- Motor Neuron Disease: Amyotrophic Lateral Sclerosis (ALS)Document2 pagesMotor Neuron Disease: Amyotrophic Lateral Sclerosis (ALS)james cordenNo ratings yet
- CTEVDocument25 pagesCTEVIceBearNo ratings yet
- Orthopedic Surgery for Knee Pain in Young GirlsDocument88 pagesOrthopedic Surgery for Knee Pain in Young Girlsteena6506763No ratings yet
- 008 Plain X-Ray AbdomenDocument7 pages008 Plain X-Ray AbdomenAthul GurudasNo ratings yet
- MSK Pathology For USMLE Step OneDocument6 pagesMSK Pathology For USMLE Step OneGrilled CroweNo ratings yet
- Clinical MnemonicsDocument23 pagesClinical MnemonicsMing WangNo ratings yet
- Amyotrophic Lateral SclerosisDocument3 pagesAmyotrophic Lateral SclerosisJohnpeter EsporlasNo ratings yet
- AV Fistula ExamDocument4 pagesAV Fistula ExamKay BristolNo ratings yet
- SC - Fracture ZMHDocument51 pagesSC - Fracture ZMHMis StromNo ratings yet
- Child With Bruises 00Document36 pagesChild With Bruises 00Awatef AbushhiwaNo ratings yet
- Dislocations and Soft Tissue InjuryDocument40 pagesDislocations and Soft Tissue InjuryAnonymousNo ratings yet
- YEAR 1 and 2 OSCE Revision: Author: DR Thomas PayneDocument30 pagesYEAR 1 and 2 OSCE Revision: Author: DR Thomas Payneminayoki100% (1)
- Last Minute Revision Points LMRPDocument4 pagesLast Minute Revision Points LMRPbetsyNo ratings yet
- Neurology NotesDocument3 pagesNeurology Notesdlynne23No ratings yet
- UKA: When Would I Do It?Document35 pagesUKA: When Would I Do It?neareastspineNo ratings yet
- PancytopeniaDocument9 pagesPancytopeniadrhammadtufailNo ratings yet
- Orthopedic SlidesDocument78 pagesOrthopedic SlidesAzry Mustapa100% (1)
- Anatomy TotalDocument19 pagesAnatomy TotalSnehanshNo ratings yet
- Ortho - Surgery PDFDocument15 pagesOrtho - Surgery PDFIC BNo ratings yet
- Slipped Capital Femoral EpiphysisDocument40 pagesSlipped Capital Femoral EpiphysisDrAshesh Desai100% (2)
- Intra Abdominal 2009Document8 pagesIntra Abdominal 2009Shinta Dwi Septiani Putri WibowoNo ratings yet
- Supracondylar FractureDocument53 pagesSupracondylar Fracturedesire kbpNo ratings yet
- Teratogens and Cardiac MalformationsDocument27 pagesTeratogens and Cardiac MalformationsNada AKNo ratings yet
- Osteomyelitis PresentationDocument15 pagesOsteomyelitis PresentationFrancis_Legasp_3667No ratings yet
- Lower Limb - Clinical AnatomyDocument18 pagesLower Limb - Clinical Anatomyewijayapala100% (2)
- Upper Limb TransDocument18 pagesUpper Limb Transashley nicholeNo ratings yet
- Clinical Pathology Case StudiesDocument10 pagesClinical Pathology Case StudiesKwadwo Sarpong JnrNo ratings yet
- Mnemonics Anatomia 1 PDFDocument11 pagesMnemonics Anatomia 1 PDFRocio SandersNo ratings yet
- Forearm & Hand AnatomyDocument5 pagesForearm & Hand AnatomyshivnairNo ratings yet
- Amboss Hemolytic AnemiaDocument16 pagesAmboss Hemolytic AnemiaAhmed Ali100% (2)
- ABC Interpretation and Pulmonary Function TestsDocument21 pagesABC Interpretation and Pulmonary Function TestsbobiomeNo ratings yet
- Bone Tumours - I & Ii - 2015Document113 pagesBone Tumours - I & Ii - 2015Nur Atiqah Mohd AzliNo ratings yet
- Spinal Cord Disease by GadisaDocument128 pagesSpinal Cord Disease by GadisaGadisa DejeneNo ratings yet
- Elbow WristDocument59 pagesElbow Wristdr_asalehNo ratings yet
- Localisation of Spinal Cord LesionsDocument218 pagesLocalisation of Spinal Cord LesionsGoh Sheen YeeNo ratings yet
- Surgery Signs, Triads N SyndromesDocument11 pagesSurgery Signs, Triads N Syndromesdrusmansaleem100% (1)
- Renal Pathology GuideDocument71 pagesRenal Pathology GuideSuha AbdullahNo ratings yet
- Cns PathologyDocument18 pagesCns Pathologysunnyorange8No ratings yet
- Synovial Chondromatosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandSynovial Chondromatosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- 6min English Kids at Home PDFDocument5 pages6min English Kids at Home PDFJim Jose AntonyNo ratings yet
- Urinary Tract Infection in Children: Dr. Alia Al-Ibrahim Consultant Pediatric Nephrology Clinical Assistant ProfessorDocument11 pagesUrinary Tract Infection in Children: Dr. Alia Al-Ibrahim Consultant Pediatric Nephrology Clinical Assistant ProfessorJim Jose AntonyNo ratings yet
- 6min English Electricity PDFDocument5 pages6min English Electricity PDFJim Jose AntonyNo ratings yet
- Common Cutaneous Infections and InfestationsDocument28 pagesCommon Cutaneous Infections and InfestationsJim Jose AntonyNo ratings yet
- Immunization in Children: Fahad Al ZamilDocument44 pagesImmunization in Children: Fahad Al ZamilJim Jose AntonyNo ratings yet
- India Today 29 June 2020 PDFDocument76 pagesIndia Today 29 June 2020 PDFJim Jose AntonyNo ratings yet
- Dr. Elham Bukhari: Aediatri Nfectious IseaseDocument56 pagesDr. Elham Bukhari: Aediatri Nfectious IseaseJim Jose AntonyNo ratings yet
- Ortho Team FinalDocument221 pagesOrtho Team FinalJim Jose AntonyNo ratings yet
- Pleural EffusionDocument10 pagesPleural EffusionJim Jose Antony100% (1)
- Strabismus, Amblyopia Management and LeukocoriaDocument19 pagesStrabismus, Amblyopia Management and LeukocoriaJim Jose AntonyNo ratings yet
- Acne Vulgaris and Acne Related DisordersDocument12 pagesAcne Vulgaris and Acne Related DisordersJim Jose AntonyNo ratings yet
- Acute Visual LossDocument10 pagesAcute Visual LossJim Jose AntonyNo ratings yet
- Refractive ErrorsDocument7 pagesRefractive ErrorsJim Jose AntonyNo ratings yet
- Optha: NeuroDocument13 pagesOptha: NeuroJim Jose AntonyNo ratings yet
- Ocular EmergenciesDocument4 pagesOcular EmergenciesJim Jose AntonyNo ratings yet
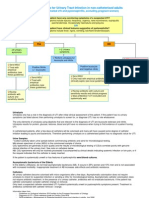
- Diagnostic Criteria For Urinary Tract InfectionDocument2 pagesDiagnostic Criteria For Urinary Tract InfectioncandyslibioNo ratings yet
- Chronic Visual LossDocument7 pagesChronic Visual LossJim Jose AntonyNo ratings yet
- COPD and BronchiectasisDocument20 pagesCOPD and BronchiectasisJim Jose AntonyNo ratings yet
- MCQ Questions May 2006Document10 pagesMCQ Questions May 2006Jim Jose AntonyNo ratings yet
- Investigations of Lung DiseasesDocument14 pagesInvestigations of Lung DiseasesJim Jose AntonyNo ratings yet
- Hair Disorders and Pigmented Skin ConditionsDocument8 pagesHair Disorders and Pigmented Skin ConditionsJim Jose AntonyNo ratings yet
- Anatomy of The Nose Nasopharynx and Paranasal Sinuses PDFDocument7 pagesAnatomy of The Nose Nasopharynx and Paranasal Sinuses PDFJim Jose AntonyNo ratings yet
- Orthopedic History Taking: DR - Kholoud Al-ZainDocument30 pagesOrthopedic History Taking: DR - Kholoud Al-ZainJim Jose AntonyNo ratings yet
- GoutDocument1 pageGoutJim Jose AntonyNo ratings yet
- Cardiology Disease List PDFDocument139 pagesCardiology Disease List PDFJim Jose AntonyNo ratings yet
- History and Physical Exam of Depressed College StudentDocument6 pagesHistory and Physical Exam of Depressed College StudentJim Jose AntonyNo ratings yet
- Medicine Annotated Multiple ChoiceDocument20 pagesMedicine Annotated Multiple ChoiceJim Jose AntonyNo ratings yet
- Paranasal SinusesDocument7 pagesParanasal SinusesJim Jose AntonyNo ratings yet
- Motor and Sensory Examination: Dr. Bandar Al Jafen, MD Consultant NeurologistDocument36 pagesMotor and Sensory Examination: Dr. Bandar Al Jafen, MD Consultant NeurologistJim Jose Antony100% (1)
- Pediatric History FormDocument2 pagesPediatric History FormJim Jose AntonyNo ratings yet
- Eladio Dieste's Free-Standing Barrel VaultsDocument18 pagesEladio Dieste's Free-Standing Barrel Vaultssoniamoise100% (1)
- Television: Operating InstructionsDocument40 pagesTelevision: Operating InstructionsNitin AgrawalNo ratings yet
- C++ Practical FileDocument15 pagesC++ Practical FilePreetish ChandraNo ratings yet
- Subtracting-Fractions-Unlike DenominatorsDocument2 pagesSubtracting-Fractions-Unlike Denominatorsapi-3953531900% (1)
- M and S Code of ConductDocument43 pagesM and S Code of ConductpeachdramaNo ratings yet
- PuppetsDocument11 pagesPuppetsShar Nur JeanNo ratings yet
- Barker-Choucalas, Vida PDFDocument176 pagesBarker-Choucalas, Vida PDFAnn GarbinNo ratings yet
- Numerical Solution of Ordinary Differential EquationsDocument31 pagesNumerical Solution of Ordinary Differential Equationschandu3072002100% (1)
- Test Engleza 8Document6 pagesTest Engleza 8Adriana SanduNo ratings yet
- 935 Ubi PBK Statement PDFDocument20 pages935 Ubi PBK Statement PDFTECHNO ACCOUNTNo ratings yet
- 457 PDFDocument8 pages457 PDFAbbey Joy CollanoNo ratings yet
- The Unseelie Prince Maze of Shadows Book 1 by Kathryn AnnDocument267 pagesThe Unseelie Prince Maze of Shadows Book 1 by Kathryn Annanissa Hri50% (2)
- Sheet Metal FormingDocument13 pagesSheet Metal FormingFranklin SilvaNo ratings yet
- Protección Fuego MetalDocument16 pagesProtección Fuego MetalTracy Mora ChNo ratings yet
- Chapter 63 Standard Integration: EXERCISE 256 Page 707Document9 pagesChapter 63 Standard Integration: EXERCISE 256 Page 707Khaerul UmamNo ratings yet
- Case NoDocument13 pagesCase NoLaurente JessicaNo ratings yet
- Oxyacetylene Welding (OAW)Document26 pagesOxyacetylene Welding (OAW)athyrahNo ratings yet
- Course Code: Hrm353 L1Document26 pagesCourse Code: Hrm353 L1Jaskiran KaurNo ratings yet
- DMGT403 Accounting For Managers PDFDocument305 pagesDMGT403 Accounting For Managers PDFpooja100% (1)
- Asset Valuation: Debt Investments: Analysis and Valuation: 1 2 N M 1 2 N MDocument23 pagesAsset Valuation: Debt Investments: Analysis and Valuation: 1 2 N M 1 2 N MSirSmirkNo ratings yet
- DRUG LISTDocument45 pagesDRUG LISTAmitKumarNo ratings yet
- MCS Adopts Milyli Software Redaction Tool BlackoutDocument3 pagesMCS Adopts Milyli Software Redaction Tool BlackoutPR.comNo ratings yet
- PP 12 Maths 2024 2Document21 pagesPP 12 Maths 2024 2Risika SinghNo ratings yet
- Admission Notice 2023-24Document2 pagesAdmission Notice 2023-24Galav PareekNo ratings yet
- Borang JPK CA 01 Tahap 2Document2 pagesBorang JPK CA 01 Tahap 2ajai1010No ratings yet
- Fisiologia de KatzDocument663 pagesFisiologia de KatzOscar Gascon100% (1)
- Isaac Asimov - "Nightfall"Document20 pagesIsaac Asimov - "Nightfall"Aditya Sharma100% (1)
- Awwa c207 Flanges Spec SheetDocument13 pagesAwwa c207 Flanges Spec SheetVincent DiepNo ratings yet
- Electronic Throttle ControlDocument67 pagesElectronic Throttle Controlmkisa70100% (1)
- CVCITC Smoke-Free Workplace Policy & ProgramDocument2 pagesCVCITC Smoke-Free Workplace Policy & ProgramKristine Joy CabujatNo ratings yet