You might also like
- EEG Neurofeedback For Treating Psychiatric DisordersDocument6 pagesEEG Neurofeedback For Treating Psychiatric DisordersAntonio PlanellesNo ratings yet
- Brain Facts - A Primer On The Brain and Nervous System 6th Edition (Malestrom) PDFDocument80 pagesBrain Facts - A Primer On The Brain and Nervous System 6th Edition (Malestrom) PDFnumuaiNo ratings yet
- Brain WavesDocument2 pagesBrain WavesAntonio PlanellesNo ratings yet
- NFB Meta Analisys Adhd Clin EEG Neurosci-2009-Arns-180-9Document11 pagesNFB Meta Analisys Adhd Clin EEG Neurosci-2009-Arns-180-9Antonio PlanellesNo ratings yet
- Neurofeedback Training Induces Changes in White and Gray MatterDocument9 pagesNeurofeedback Training Induces Changes in White and Gray MatterEdward NoriaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 4BE0 01 Rms BengaliDocument13 pages4BE0 01 Rms BengaliJohn HopkinsNo ratings yet
- Leadership Compass ActivityDocument5 pagesLeadership Compass ActivityPsiho LoguseNo ratings yet
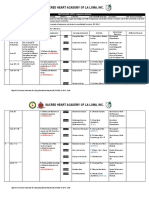
- Curriculum Map Grade 10 2019 2020Document15 pagesCurriculum Map Grade 10 2019 2020Sacred Heart Academy of La Loma100% (1)
- Lucas, Marinella JDocument1 pageLucas, Marinella JMarinella LucasNo ratings yet
- Week 4 2ND Quarter English 8 Marionne BagtasDocument7 pagesWeek 4 2ND Quarter English 8 Marionne BagtasMarionne Aleigne BagtasNo ratings yet
- The Racial Complex: A Jungian Perspective - Fanny BrewsterDocument143 pagesThe Racial Complex: A Jungian Perspective - Fanny BrewsterAlgumCaraNo ratings yet
- Sumarry 1 - The Mindful Music EducatorDocument1 pageSumarry 1 - The Mindful Music EducatorAngela GohNo ratings yet
- Education, Summer Camps and Programs - 0215WKTDocument10 pagesEducation, Summer Camps and Programs - 0215WKTtimesnewspapersNo ratings yet
- Literature Review GeographyDocument7 pagesLiterature Review Geographyafmzinuvouzeny100% (1)
- Hydrologic AnalysisDocument3 pagesHydrologic AnalysisHendroNo ratings yet
- Mygov 1704534118122933441Document5 pagesMygov 1704534118122933441anvu4848No ratings yet
- Communicating EffectivelyDocument3 pagesCommunicating EffectivelyHanna Vin JuezanNo ratings yet
- CHAPTER 2: Data Collection and Basic Concepts in Sampling DesignDocument14 pagesCHAPTER 2: Data Collection and Basic Concepts in Sampling DesignDominique Anne BenozaNo ratings yet
- Document Without A Written Permission From Lam-Ang Publishing Is Strictly ProhibitedDocument6 pagesDocument Without A Written Permission From Lam-Ang Publishing Is Strictly Prohibitedryan mascariñasNo ratings yet
- Q3L2 HomeworkDocument3 pagesQ3L2 HomeworkTrung PhamNo ratings yet
- RA Criminologists Davao June2019 PDFDocument102 pagesRA Criminologists Davao June2019 PDFPhilBoardResultsNo ratings yet
- The Da Vinci Studio School of Science and EngineeringDocument20 pagesThe Da Vinci Studio School of Science and EngineeringNHCollegeNo ratings yet
- Afbba 7Document14 pagesAfbba 7Yasmin SantanaNo ratings yet
- Agile Fundamentals Learning OutcomesDocument11 pagesAgile Fundamentals Learning OutcomesGabriela Venegas100% (1)
- Mtech 2013 RankDocument419 pagesMtech 2013 Ranksatyendra_scribd81No ratings yet
- Unit 11 - Strategic Quality and Systems ManagementDocument4 pagesUnit 11 - Strategic Quality and Systems ManagementEYmran RExa XaYdi100% (1)
- 9-16-20 Assessments in Special Education Power PTDocument32 pages9-16-20 Assessments in Special Education Power PTHiba BarakatNo ratings yet
- Science 10 - Q3 - W6 - D2Document2 pagesScience 10 - Q3 - W6 - D2zenaida a academiaNo ratings yet
- Building Your Dream Canadian 10th Edition Good Solutions ManualDocument28 pagesBuilding Your Dream Canadian 10th Edition Good Solutions ManualAngelaKnapptndrj100% (16)
- Required Officer Like Qualities OLQs For Passing SSB InterviewsDocument2 pagesRequired Officer Like Qualities OLQs For Passing SSB InterviewsSaahiel SharrmaNo ratings yet
- IMU-UG Admission RanksDocument441 pagesIMU-UG Admission RanksParth JhaNo ratings yet
- Personal Growth-Building HabitsDocument3 pagesPersonal Growth-Building HabitsMr. QuitNo ratings yet
- Karnataka State Excise SubDocument7 pagesKarnataka State Excise SubCHETANNo ratings yet
- Equivalent Concept - Titration APSPDocument20 pagesEquivalent Concept - Titration APSPBeena JayNo ratings yet
- 2 Field Study Activities 7Document13 pages2 Field Study Activities 7Dionisia Rosario CabrillasNo ratings yet