You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- EstimatingDocument309 pagesEstimatingFauzankalibata92% (24)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Scientific American - February 2019Document112 pagesScientific American - February 2019Frankling AguilarNo ratings yet
- The Effect of Unbalance On Bearing LifeDocument8 pagesThe Effect of Unbalance On Bearing LifejaypallaNo ratings yet
- Curtiss SO3C-1 Seamew Recon PlaneDocument11 pagesCurtiss SO3C-1 Seamew Recon PlaneAdrian Rosero Bautista100% (1)
- Guidelines For Noise Labelling and Emission Limits of Outdoor Sources 2nd Edition 2007Document30 pagesGuidelines For Noise Labelling and Emission Limits of Outdoor Sources 2nd Edition 2007sl1828No ratings yet
- GM Construction Leads Rs 8140 Crore PCII C2C3 Recovery ProjectDocument24 pagesGM Construction Leads Rs 8140 Crore PCII C2C3 Recovery ProjectAnuj GuptaNo ratings yet
- Siemens Compressor PackageDocument8 pagesSiemens Compressor PackageMilos ObrenovicNo ratings yet
- 7 Geolog Drilling Optimization ServicesDocument10 pages7 Geolog Drilling Optimization ServicespendexxNo ratings yet
- Equalities Act Schedule 8 - Article 24Document5 pagesEqualities Act Schedule 8 - Article 24LibbyDrakeNo ratings yet
- All I Ask A Capella - Click Structure - TENOR 1Document3 pagesAll I Ask A Capella - Click Structure - TENOR 1LibbyDrakeNo ratings yet
- SurvivalDocument26 pagesSurvivalLibbyDrakeNo ratings yet
- Tudornurseryrhymes 6Document8 pagesTudornurseryrhymes 6xxxfarahxxxNo ratings yet
- SBT Poster Form ThanetDocument2 pagesSBT Poster Form ThanetLibbyDrakeNo ratings yet
- TH3122 004 PDFDocument14 pagesTH3122 004 PDFSasa MitrovicNo ratings yet
- Spreading Sequences: Tan F. Wong: Spread Spectrum & CDMADocument23 pagesSpreading Sequences: Tan F. Wong: Spread Spectrum & CDMAadeeb_2006No ratings yet
- Lateral Earth Pressures For Seismic Design of Cantilever Retaining WallsDocument8 pagesLateral Earth Pressures For Seismic Design of Cantilever Retaining Wallsredpol100% (2)
- D 2320 - 98 R03 RdizmjaDocument3 pagesD 2320 - 98 R03 RdizmjaEliKax!No ratings yet
- Bennett, Stuart Virk, Gurvinder S Computer Control of Real-Time ProcessesDocument322 pagesBennett, Stuart Virk, Gurvinder S Computer Control of Real-Time ProcessesPTR77No ratings yet
- Electronics Media Internship Report ZEE NEWS CGDocument15 pagesElectronics Media Internship Report ZEE NEWS CGPrashant PandyaNo ratings yet
- Presentation Title: Debugging Simulation ModelsDocument74 pagesPresentation Title: Debugging Simulation ModelsflyingdreamsNo ratings yet
- R&D Lorenzo-Siciliano ENIDocument11 pagesR&D Lorenzo-Siciliano ENIinterponNo ratings yet
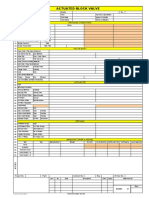
- DSS2060D Actuated Block Valve DatasheetDocument1 pageDSS2060D Actuated Block Valve Datasheetkrishna kumarNo ratings yet
- B.Tech Machine Design SyllabusDocument25 pagesB.Tech Machine Design SyllabusSanketHedduriNo ratings yet
- Fluid Mechanics CalculationsDocument3 pagesFluid Mechanics CalculationsandreagassiNo ratings yet
- w13 - CRM How It Works and Help BusinessDocument15 pagesw13 - CRM How It Works and Help BusinessYahya Vernanda RamadhaniNo ratings yet
- Manual en Español Kip 3000Document2 pagesManual en Español Kip 3000Ja De OstiaNo ratings yet
- Joybook A52 Series EnglishDocument44 pagesJoybook A52 Series EnglishTudor VladNo ratings yet
- Sunstack Tech SpecDocument2 pagesSunstack Tech SpecAdriel MirtoNo ratings yet
- Smart Selangor Briefing and Invitation to Express InterestDocument30 pagesSmart Selangor Briefing and Invitation to Express InterestKUSATEX AZMI0% (1)
- Lobbying Vacations For CongressDocument54 pagesLobbying Vacations For CongressBigMamaTEANo ratings yet
- JMeter OAuth SamplerDocument3 pagesJMeter OAuth SamplerFredy NataNo ratings yet
- FS7M0680, FS7M0880: Fairchild Power Switch (FPS)Document19 pagesFS7M0680, FS7M0880: Fairchild Power Switch (FPS)Arokiaraj RajNo ratings yet
- RemoteDocument16 pagesRemotetok222222No ratings yet
- BassoonBocals PDFDocument3 pagesBassoonBocals PDFnheyminkNo ratings yet
- Print to PDF without novaPDF messageDocument60 pagesPrint to PDF without novaPDF messageAyush GuptaNo ratings yet