You might also like
- Uwb Radar Signal Processing For Through The WallDocument20 pagesUwb Radar Signal Processing For Through The WallJaipreet SinghNo ratings yet
- Software Radio and The Future of Wireless Security: Michael Ossmann Institute For Telecommunication SciencesDocument62 pagesSoftware Radio and The Future of Wireless Security: Michael Ossmann Institute For Telecommunication SciencesGopa Kumar100% (1)
- LASER CommunicationDocument16 pagesLASER CommunicationarjunknarayanNo ratings yet
- Communication Networks Leon Garcia PDF DownloadDocument3 pagesCommunication Networks Leon Garcia PDF DownloadSudesh Agrawal0% (3)
- Amateur's Guide to Getting Started with Software Defined Radio (SDRDocument32 pagesAmateur's Guide to Getting Started with Software Defined Radio (SDRJos1No ratings yet
- Laser Based Communication LinkDocument90 pagesLaser Based Communication LinkSaurabh Kolhe100% (1)
- Basic Calculation of A Boost Converter's Power StageDocument9 pagesBasic Calculation of A Boost Converter's Power Stagexuanvan1303No ratings yet
- Active Directory Tutorial: Learn the Basics of Microsoft's Directory ServiceDocument46 pagesActive Directory Tutorial: Learn the Basics of Microsoft's Directory ServiceSarwer PatelNo ratings yet
- LTE Actix Drive ReportDocument120 pagesLTE Actix Drive ReportPranjulDwivediNo ratings yet
- KPDX (Portland Intl) - R (04feb16) PDFDocument40 pagesKPDX (Portland Intl) - R (04feb16) PDFnabatman100% (1)
- Chapter 4: SQL: ©silberschatz, Korth and Sudarshan 4.1 Database System ConceptsDocument98 pagesChapter 4: SQL: ©silberschatz, Korth and Sudarshan 4.1 Database System Conceptscap2010No ratings yet
- DVB-S2/RCS Mesh Networking for Rural Telephone AccessDocument15 pagesDVB-S2/RCS Mesh Networking for Rural Telephone AccessAbood AlakhrasNo ratings yet
- 04 Ie437Document10 pages04 Ie437VijendraSinghTomarNo ratings yet
- Software Defined Radios in S Atellite Communication: Trident Academy of TechnologyDocument21 pagesSoftware Defined Radios in S Atellite Communication: Trident Academy of Technology108databoxNo ratings yet
- MX300 Maint Manual-Complete 2-09Document148 pagesMX300 Maint Manual-Complete 2-09Pastor Hernández JacintoNo ratings yet
- RF, and Microwaves in Medicine and Biology, (Doi:: 10.1109/JERM.2020.3026588Document16 pagesRF, and Microwaves in Medicine and Biology, (Doi:: 10.1109/JERM.2020.3026588Generation GenerationNo ratings yet
- Software Radio: An Emerging Technology in Wireless CommunicationDocument9 pagesSoftware Radio: An Emerging Technology in Wireless Communicationaravind44555No ratings yet
- CWNA Guide To Wireless LANs, Second Edition - Ch1Document3 pagesCWNA Guide To Wireless LANs, Second Edition - Ch1NickHenry100% (1)
- DSP in RadarDocument11 pagesDSP in RadarSon Vo PhiNo ratings yet
- Radio PillDocument41 pagesRadio PillAadhithya Priya100% (2)
- Smart Antenna Full ReportDocument9 pagesSmart Antenna Full ReportPriyanka Kushwaha100% (1)
- Free Space Laser CommunicationDocument19 pagesFree Space Laser CommunicationSourav Sahoo100% (1)
- Magic MonitorDocument178 pagesMagic MonitorAbdul LateefNo ratings yet
- Final Project ReportDocument81 pagesFinal Project ReportZeeshan AhmadNo ratings yet
- Low Cost Prototype Simulation of Spectrum Analyzer Base On GNU Radio and RTL-SDRDocument13 pagesLow Cost Prototype Simulation of Spectrum Analyzer Base On GNU Radio and RTL-SDRBambang Bagus HariantoNo ratings yet
- Mesh Topology ReportDocument27 pagesMesh Topology ReportRahul Garg100% (1)
- Thaens - NATO Cooperative ESM OperationsDocument11 pagesThaens - NATO Cooperative ESM OperationsMartin Schweighart MoyaNo ratings yet
- GBPPR Active Denial SystemDocument30 pagesGBPPR Active Denial SystemRobert EckardtNo ratings yet
- Wireless Voice Communication Using LaserDocument2 pagesWireless Voice Communication Using Laserthiyagar_6100% (4)
- Alcatel Lucent 9400 AWyDocument6 pagesAlcatel Lucent 9400 AWyLan Twin SummerNo ratings yet
- The Relative Nature of Low Probability of Detection Radar: A Countermeasures PerspectiveDocument36 pagesThe Relative Nature of Low Probability of Detection Radar: A Countermeasures PerspectiveamenendezamNo ratings yet
- QoS Issues With Focus On Wireless Body Area NetworksDocument7 pagesQoS Issues With Focus On Wireless Body Area NetworksTabassumWaheedNo ratings yet
- Narrowband Iot Usrp WP LTR WRDocument14 pagesNarrowband Iot Usrp WP LTR WRSkadik 202 SlmNo ratings yet
- Pelicanhpc: A Linux Cluster Distribution For Mpi-Based Parallel ComputingDocument9 pagesPelicanhpc: A Linux Cluster Distribution For Mpi-Based Parallel ComputingforwalrusNo ratings yet
- PICAXE Powered CW BeaconsDocument7 pagesPICAXE Powered CW BeaconsAmp AunyamoneNo ratings yet
- TELOSB MOTE PLATFORM SPECSDocument2 pagesTELOSB MOTE PLATFORM SPECSRaj Gaurav Mishra100% (1)
- Exercise Chap 2Document3 pagesExercise Chap 2chantinh_hd190No ratings yet
- Application Note Usrp and HDSDR Spectrum MonitoringDocument14 pagesApplication Note Usrp and HDSDR Spectrum MonitoringcaraboyNo ratings yet
- CSTD-104-439 - Simulation of Wearable Antennas For Body Centric Wireless Communications (Repaired)Document56 pagesCSTD-104-439 - Simulation of Wearable Antennas For Body Centric Wireless Communications (Repaired)Sandhya PandeyNo ratings yet
- (Sawan, Salam, Et All) Wireless Recording Systems From Noninvasive EEG-NIRS To Invasive EEG DevicesDocument10 pages(Sawan, Salam, Et All) Wireless Recording Systems From Noninvasive EEG-NIRS To Invasive EEG DevicesJoana Marini De Oliveira CoutoNo ratings yet
- Wireless Mesh Networking: A 40-Character TitleDocument13 pagesWireless Mesh Networking: A 40-Character TitleJoker's WorldNo ratings yet
- Super Wi-FiDocument15 pagesSuper Wi-FiMary BinithaNo ratings yet
- Xmax SeminarDocument24 pagesXmax SeminarGirish ChouguleNo ratings yet
- Getting Startted With GNU Radio and USRPDocument6 pagesGetting Startted With GNU Radio and USRPAdeel AhmadNo ratings yet
- 07 Chapter2Document13 pages07 Chapter2Arslan AliNo ratings yet
- BiotelemetryDocument22 pagesBiotelemetryapi-375783880% (5)
- Manual Ni Usrp 2920Document56 pagesManual Ni Usrp 2920Anghye Plata100% (1)
- One Way of Getting 3D Buildings Into ATAKDocument5 pagesOne Way of Getting 3D Buildings Into ATAKfoxbat1988No ratings yet
- EETimes July-August 2012Document56 pagesEETimes July-August 2012Brzata PticaNo ratings yet
- IMDDocument111 pagesIMDTwintu VinishNo ratings yet
- Mobile Computing: Introduction:: Unit - IDocument4 pagesMobile Computing: Introduction:: Unit - IA MNo ratings yet
- Mwjournalmwj201312 DLDocument124 pagesMwjournalmwj201312 DLm_magdiNo ratings yet
- Spectral Analysis With RTL-SDR RadioDocument2 pagesSpectral Analysis With RTL-SDR RadioDramane BonkoungouNo ratings yet
- C++ GnuradioDocument23 pagesC++ Gnuradionadeemp78No ratings yet
- TOSN LoRaDocument35 pagesTOSN LoRaprabhu_natarajan_nNo ratings yet
- Ieee Research Paper On Brain Computer InterfaceDocument10 pagesIeee Research Paper On Brain Computer Interfacefvgy6fn3100% (1)
- Microwave Range FinderDocument54 pagesMicrowave Range FinderNivethithaa DhanrajNo ratings yet
- Simple Structure Multiband Patch Antenna With Three SlotsDocument3 pagesSimple Structure Multiband Patch Antenna With Three SlotsSabah ShamsNo ratings yet
- Brain Reading: How National Security Could Gain Access to Our BrainsFrom EverandBrain Reading: How National Security Could Gain Access to Our BrainsNo ratings yet
- A Compact Implantable MIMO Antenna For High-Data-Rate Biotelemetry ApplicationsDocument10 pagesA Compact Implantable MIMO Antenna For High-Data-Rate Biotelemetry Applicationsgf.msaniNo ratings yet
- Implantable Antennas For Bio-Medical ApplicationsDocument16 pagesImplantable Antennas For Bio-Medical ApplicationseladNo ratings yet
- Articulo Implante Antenas MiniDocument9 pagesArticulo Implante Antenas MiniseykarimNo ratings yet
- Dual-Band Two-Port MIMO Antenna For Biomedical Deep Tissue Communication Design Characterization and Performance AnalysisDocument11 pagesDual-Band Two-Port MIMO Antenna For Biomedical Deep Tissue Communication Design Characterization and Performance AnalysisJamal Abdul NasyirNo ratings yet
- Wearable Conformal Antennas For 2.4 GHZ Wireless Body Area NetworksDocument7 pagesWearable Conformal Antennas For 2.4 GHZ Wireless Body Area NetworksSpagnuolo Domenico PioNo ratings yet
- Mirrored Coupling Structures For Microwave Signal Splitting and Combining PDFDocument6 pagesMirrored Coupling Structures For Microwave Signal Splitting and Combining PDFagmnm1962No ratings yet
- Scr's & Triacs Cross ReferenceDocument11 pagesScr's & Triacs Cross Referenceagmnm1962No ratings yet
- 12 G To 20 G Compact Rectangle Waveguide To Circular Waveguide Mode ConvertorDocument2 pages12 G To 20 G Compact Rectangle Waveguide To Circular Waveguide Mode Convertoragmnm1962No ratings yet
- Broadband Lumped-Element Integrated - Way Power Dividers For Voltage StandardsDocument9 pagesBroadband Lumped-Element Integrated - Way Power Dividers For Voltage Standardsagmnm1962No ratings yet
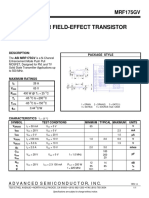
- MRF 175 GVDocument1 pageMRF 175 GVagmnm1962No ratings yet
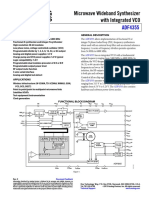
- ADF4355 54-6800 MHZ Microwave Wideband Synthesizer With Integrated VCODocument35 pagesADF4355 54-6800 MHZ Microwave Wideband Synthesizer With Integrated VCOagmnm1962No ratings yet
- ACS712 Demo Board Guide PDFDocument11 pagesACS712 Demo Board Guide PDFagmnm1962No ratings yet
- High Power CombinerDocument5 pagesHigh Power Combineragmnm1962No ratings yet
- 51W 10540 1Document16 pages51W 10540 1Mitrofan AnduNo ratings yet
- Patch Antenna Design MAnualDocument36 pagesPatch Antenna Design MAnualkarthikvel_852246No ratings yet
- A Compact Ultra-Wideband Power Divider With High Isolation 3.1-10.6 GHZDocument2 pagesA Compact Ultra-Wideband Power Divider With High Isolation 3.1-10.6 GHZagmnm1962No ratings yet
- 200watt Active Load UnitDocument14 pages200watt Active Load Unitagmnm1962No ratings yet
- A Novel Wideband Bandpass Power Divider With Harmonic Suppressed Ring Resonator 1.41-2.68 GHZDocument4 pagesA Novel Wideband Bandpass Power Divider With Harmonic Suppressed Ring Resonator 1.41-2.68 GHZagmnm1962No ratings yet
- AN5142 Radio Link-Budget Calculations For ISM-RF ProductsDocument11 pagesAN5142 Radio Link-Budget Calculations For ISM-RF Productsagmnm1962No ratings yet
- DB3 DB4 SMDB3 - Diac PDFDocument6 pagesDB3 DB4 SMDB3 - Diac PDFmsicoie1851No ratings yet
- C106BOS Datasheetz PDFDocument6 pagesC106BOS Datasheetz PDFAnonymous na7OSZaNo ratings yet
- Tipl762 - NPN Silicon Power TransistorsDocument7 pagesTipl762 - NPN Silicon Power Transistorsagmnm1962No ratings yet
- Data Sheet: UHF Push-Pull Power MOS TransistorDocument15 pagesData Sheet: UHF Push-Pull Power MOS Transistoragmnm1962No ratings yet
- tl783 PDFDocument26 pagestl783 PDFLuiz CaldeiraNo ratings yet
- Variable High Voltage BJT Regulator User ManualDocument7 pagesVariable High Voltage BJT Regulator User Manualagmnm1962No ratings yet
- SP 500 SpecDocument2 pagesSP 500 Specagmnm1962No ratings yet
- SP431 Adjustable Precision RegulatorsDocument11 pagesSP431 Adjustable Precision Regulatorsagmnm1962No ratings yet
- Sprabw0b PDFDocument19 pagesSprabw0b PDFAshok KumarNo ratings yet
- Testing A Power Supply For Line and Load TransientsDocument7 pagesTesting A Power Supply For Line and Load Transientsagmnm1962No ratings yet
- Creating A Fast Load TransientDocument3 pagesCreating A Fast Load Transientagmnm1962No ratings yet
- Pads WhitepaperDocument23 pagesPads Whitepaperagmnm1962No ratings yet
- Design of a 2.5kW isolated DC/DC fullbridge converter for electric vehicle applicationDocument55 pagesDesign of a 2.5kW isolated DC/DC fullbridge converter for electric vehicle applicationmarconi-agNo ratings yet
- LXA-7500 Series X-Band Low Noise AmplifiersDocument4 pagesLXA-7500 Series X-Band Low Noise Amplifiersagmnm1962No ratings yet
- TDJ 609015DEI 65Fv01Document1 pageTDJ 609015DEI 65Fv01辛凯No ratings yet
- Transmission Modes and Beamforming in LTEDocument16 pagesTransmission Modes and Beamforming in LTEwizards witchNo ratings yet
- Pakistan Satellite ListDocument69 pagesPakistan Satellite Listghaffar100% (3)
- BGWTsbupQdyLOVFtaIZw - Elexon Mining - Cave-Block Cave Mine MonitoringDocument14 pagesBGWTsbupQdyLOVFtaIZw - Elexon Mining - Cave-Block Cave Mine MonitoringJuan MedinaNo ratings yet
- Hasan Bin Firoz Communication TheoryDocument20 pagesHasan Bin Firoz Communication TheorySiam hasanNo ratings yet
- DB411-B Product Specifications (Comprehensive)Document3 pagesDB411-B Product Specifications (Comprehensive)Jhady BolivarNo ratings yet
- V 01Document2 pagesV 01marco100% (1)
- DX-790-960-65-16.5i-M: Electrical PropertiesDocument2 pagesDX-790-960-65-16.5i-M: Electrical PropertiesMadalina Jarii0% (1)
- DTH Satellite Advantages Over Cable TVDocument4 pagesDTH Satellite Advantages Over Cable TVManish GoyalNo ratings yet
- LinkBudget 1Document8 pagesLinkBudget 1Achintha AluthmanageNo ratings yet
- Wise MacDocument36 pagesWise MacivanNo ratings yet
- SKBO VOR Rwy 13RDocument1 pageSKBO VOR Rwy 13RBobNo ratings yet
- How To Make Successful Wifi 6 PocDocument24 pagesHow To Make Successful Wifi 6 PocYasmine BoudhinaNo ratings yet
- Update on the Latest Release of IEC 61000-4-3 Edition 3Document9 pagesUpdate on the Latest Release of IEC 61000-4-3 Edition 3LOUKILkarimNo ratings yet
- CiscoDocument36 pagesCiscoYoelNo ratings yet
- Dxxx-690-960/1695-2690/1695-2690-65/65/65-16I/18I/18I-M/M/M-R Easyret 6-Port Antenna With 3 Integrated Rcus - 2.0M Model: Atr4518R6V06Document2 pagesDxxx-690-960/1695-2690/1695-2690-65/65/65-16I/18I/18I-M/M/M-R Easyret 6-Port Antenna With 3 Integrated Rcus - 2.0M Model: Atr4518R6V06Дмитрий СпиридоновNo ratings yet
- Trimble r7 Gnss Datasheet PDFDocument2 pagesTrimble r7 Gnss Datasheet PDFRomi RiskiNo ratings yet
- Zte 2g AlarmDocument1 pageZte 2g AlarmDash DungaNo ratings yet
- WRS15-small Satellites-06122018 PDFDocument56 pagesWRS15-small Satellites-06122018 PDFFunke Oni-alaoNo ratings yet
- SMR SMC RP Data CP DataDocument127 pagesSMR SMC RP Data CP DataaxebcNo ratings yet
- Test Report BT Classics 3988475Document35 pagesTest Report BT Classics 3988475Scott RothrockNo ratings yet
- Eh Antenna DesignDocument2 pagesEh Antenna DesignYayok S. AnggoroNo ratings yet
- Drive Test Analysis - A Case StudyDocument21 pagesDrive Test Analysis - A Case Studygchivandire100% (7)
- Cispr TR 16-4-4-2007Document64 pagesCispr TR 16-4-4-2007石明桀No ratings yet
- Design and Simulation of Different Types of Antenna Using MatlabDocument12 pagesDesign and Simulation of Different Types of Antenna Using MatlabChandra shekara mnNo ratings yet
- Introduction To Radar Scattering Application in ReDocument17 pagesIntroduction To Radar Scattering Application in ReGemmy94No ratings yet
- Ultimate Maritime Radio TesterDocument2 pagesUltimate Maritime Radio TestereminNo ratings yet