You might also like
- Anna Rozaliyani: Department of Parasitology-Faculty of Medicine, Universitas IndonesiaDocument27 pagesAnna Rozaliyani: Department of Parasitology-Faculty of Medicine, Universitas Indonesiainka.elseNo ratings yet
- Introduction To Molecular Biology (Unib 2010)Document59 pagesIntroduction To Molecular Biology (Unib 2010)inka.elseNo ratings yet
- Gene Expression Regulation of Procaryotes & Viruses: Fera Ibrahim & T. Mirawati Sudiro Departemen Mikrobiologi FkuiDocument80 pagesGene Expression Regulation of Procaryotes & Viruses: Fera Ibrahim & T. Mirawati Sudiro Departemen Mikrobiologi Fkuiinka.elseNo ratings yet
- Physiology of the Thyroid GlandDocument35 pagesPhysiology of the Thyroid Glandinka.elseNo ratings yet
- Physiology of the Thyroid GlandDocument35 pagesPhysiology of the Thyroid Glandinka.elseNo ratings yet
- Identifikasi Staphylococcus Aureus Penyebab Mastitis Dengan Uji Fermentasi Mannitol Dan Deteksi PDocument12 pagesIdentifikasi Staphylococcus Aureus Penyebab Mastitis Dengan Uji Fermentasi Mannitol Dan Deteksi PNita YesitaNo ratings yet
- Intro Tothe Function of Parathyroid Gland, ConciseDocument34 pagesIntro Tothe Function of Parathyroid Gland, Conciseinka.elseNo ratings yet
- Introduction To The Endocrine Control On MetabolismDocument79 pagesIntroduction To The Endocrine Control On Metabolisminka.elseNo ratings yet
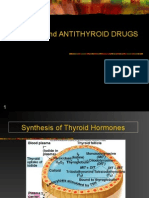
- Thyroid and Antithyroid DrugsDocument49 pagesThyroid and Antithyroid Drugsinka.elseNo ratings yet
- 07 3857research0210 35 40Document6 pages07 3857research0210 35 40inka.elseNo ratings yet
- NagaokaDocument13 pagesNagaokainka.elseNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 10.2 - RheumatologyDocument40 pages10.2 - Rheumatologyayeshafarooq60No ratings yet
- Overcoming Arthritis - 5th Revised Edition E-BookDocument89 pagesOvercoming Arthritis - 5th Revised Edition E-Bookmike davis100% (6)
- Rheumatology Clinical Scenarios Ebook p2gnjrDocument60 pagesRheumatology Clinical Scenarios Ebook p2gnjrAleeza khanNo ratings yet
- NEW Online Exam Guideline 2020Document87 pagesNEW Online Exam Guideline 2020arezooNo ratings yet
- Pediatric Specialists - Managing The Medical MazeDocument4 pagesPediatric Specialists - Managing The Medical MazePathways AwarenessNo ratings yet
- Set 5, Reumatology, ArpanaDocument14 pagesSet 5, Reumatology, ArpanaSahana hadaNo ratings yet
- Oxford Textbook of Musculoskeletal Medicine (2nd Edition) : The Journal of Rheumatology June 2016Document3 pagesOxford Textbook of Musculoskeletal Medicine (2nd Edition) : The Journal of Rheumatology June 2016RiaFernandesNo ratings yet
- Health 10 - Q1 - Module1aDocument18 pagesHealth 10 - Q1 - Module1aphotomusicianNo ratings yet
- ArthritisDocument406 pagesArthritiskikria100% (2)
- Mycoplasmic Theory of Rheumatoid DiseaseDocument81 pagesMycoplasmic Theory of Rheumatoid DiseaseChristopher Phillips100% (1)
- Fajo 990Document238 pagesFajo 990Mohamed A SalehNo ratings yet
- UK Rheumatology Training 2021Document32 pagesUK Rheumatology Training 2021SmallsNo ratings yet
- Dr. Antonious S. Hanna: General Practitioner Experience - . - 10 YearsDocument29 pagesDr. Antonious S. Hanna: General Practitioner Experience - . - 10 YearsdoctorantoniNo ratings yet
- The New Age Family HospitalDocument5 pagesThe New Age Family HospitalPooja HariNo ratings yet
- Hand Exercise For Women With Rheumatoid Arthritis and Decreased Hand Function: An Exploratory Randomized Controlled TrialDocument9 pagesHand Exercise For Women With Rheumatoid Arthritis and Decreased Hand Function: An Exploratory Randomized Controlled TrialrohanaNo ratings yet
- Dr. Laniyati-Autoimun Prodia 29 April 2018 PDFDocument23 pagesDr. Laniyati-Autoimun Prodia 29 April 2018 PDFNururrohmahNo ratings yet
- MRCP Syllabus-1Document19 pagesMRCP Syllabus-1Medico HubNo ratings yet
- Assessment FormDocument8 pagesAssessment FormbonnieyfNo ratings yet
- Edukasi Kesehatan Tentang Pencegahan GoutDocument4 pagesEdukasi Kesehatan Tentang Pencegahan GoutuiNo ratings yet
- Nodular Rheumatoid Arthritis Resembling Gout: Katrina Chakradeo, Katie Buzacott, Muriel SodenDocument2 pagesNodular Rheumatoid Arthritis Resembling Gout: Katrina Chakradeo, Katie Buzacott, Muriel SodenrhizkyNo ratings yet
- Journal of Clinical Rheumatology, Panlar 2012 PDFDocument44 pagesJournal of Clinical Rheumatology, Panlar 2012 PDFTuliaStellaNo ratings yet
- 61 FullDocument8 pages61 FullAndreiMunteanuNo ratings yet
- On Rheumatic FeverDocument30 pagesOn Rheumatic Feverkiran kumari yadav100% (1)
- The ANA Test: All You Need To KnowDocument14 pagesThe ANA Test: All You Need To KnowJackeline DoigNo ratings yet
- Poster Number Name Country Remarks TitleDocument26 pagesPoster Number Name Country Remarks TitleAndy F Monroe0% (1)
- Rheuma Prestests CompiledDocument13 pagesRheuma Prestests CompiledJolaine ValloNo ratings yet
- Nicola Zammitt, - Alastair O'Brien - Essentials of Kumar & Clark's Clinical Medicine-Elsevier (2017) PDFDocument927 pagesNicola Zammitt, - Alastair O'Brien - Essentials of Kumar & Clark's Clinical Medicine-Elsevier (2017) PDFJamie Baczewski100% (8)
- Partners and Nurses' Knowledge and Representations of Gout: A Qualitative StudyDocument8 pagesPartners and Nurses' Knowledge and Representations of Gout: A Qualitative Studyharfiana safitri08No ratings yet
- 17 Aususgt Final ProtocolDocument22 pages17 Aususgt Final ProtocolRishabh VermaNo ratings yet
- Bhagat2019 PDFDocument7 pagesBhagat2019 PDFsita nur annisa100% (1)