You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Case DiscussionDocument8 pagesCase DiscussionAishwarya BharathNo ratings yet
- Conflict Resolution Lesson Plan PDFDocument2 pagesConflict Resolution Lesson Plan PDFapi-448873912No ratings yet
- Blood CollectionDocument25 pagesBlood Collectionطاهرة حربية AlcaldeNo ratings yet
- Self Help For PanicDocument10 pagesSelf Help For PanicIqbal Baryar100% (1)
- Annals of Surgery Volume 257 Issue 6 2013 (Doi 10.1097/sla.0b013e31826eda3b) Iida, Tomohiko Nomori, Hiroaki Shiba, Mitsutoshi Nakajima, Ju - Prognostic Factors After Pulmonary Metastasectomy ForDocument6 pagesAnnals of Surgery Volume 257 Issue 6 2013 (Doi 10.1097/sla.0b013e31826eda3b) Iida, Tomohiko Nomori, Hiroaki Shiba, Mitsutoshi Nakajima, Ju - Prognostic Factors After Pulmonary Metastasectomy ForNurul Dwi UtamiNo ratings yet
- CA Recti Pulmonal MetastasisDocument7 pagesCA Recti Pulmonal MetastasisNurul Dwi UtamiNo ratings yet
- Suicide Risk of Depressed PatientDocument6 pagesSuicide Risk of Depressed PatientNurul Dwi UtamiNo ratings yet
- International Journal of Clinical Oncology Volume 17 Issue 1 2012 (Doi 10.1007/s10147-011-0315-2) Toshiaki Watanabe Michio Itabashi Yasuhiro Shimada Shinji Tan - Japanese Society For Cancer of T PDFDocument29 pagesInternational Journal of Clinical Oncology Volume 17 Issue 1 2012 (Doi 10.1007/s10147-011-0315-2) Toshiaki Watanabe Michio Itabashi Yasuhiro Shimada Shinji Tan - Japanese Society For Cancer of T PDFNurul Dwi UtamiNo ratings yet
- Metastatic Pattern of Colorectal CarcinomaDocument7 pagesMetastatic Pattern of Colorectal CarcinomaNurul Dwi UtamiNo ratings yet
- Metastatic Colorectal CancerDocument9 pagesMetastatic Colorectal CancerNurul Dwi UtamiNo ratings yet
- Survival After Lung Metastasectomy in Colorectal Cancer Patients With Previously Resected Liver MetastasesDocument6 pagesSurvival After Lung Metastasectomy in Colorectal Cancer Patients With Previously Resected Liver MetastasesNurul Dwi UtamiNo ratings yet
- International Journal of Clinical Oncology Volume 17 Issue 1 2012 (Doi 10.1007/s10147-011-0315-2) Toshiaki Watanabe Michio Itabashi Yasuhiro Shimada Shinji Tan - Japanese Society For Cancer of T PDFDocument29 pagesInternational Journal of Clinical Oncology Volume 17 Issue 1 2012 (Doi 10.1007/s10147-011-0315-2) Toshiaki Watanabe Michio Itabashi Yasuhiro Shimada Shinji Tan - Japanese Society For Cancer of T PDFNurul Dwi UtamiNo ratings yet
- Lung CancerDocument11 pagesLung CancerNurul Dwi UtamiNo ratings yet
- Lung CancerDocument11 pagesLung CancerNurul Dwi UtamiNo ratings yet
- Effect of Environment To Colorectal CarcinomaDocument14 pagesEffect of Environment To Colorectal CarcinomaNurul Dwi UtamiNo ratings yet
- Fasting Enhances Cancer TherapyDocument9 pagesFasting Enhances Cancer TherapyNurul Dwi Utami100% (1)
- Radiofrequency TreatmentDocument5 pagesRadiofrequency TreatmentNurul Dwi UtamiNo ratings yet
- Neuroblastoma PDFDocument5 pagesNeuroblastoma PDFHanna G. FauziaNo ratings yet
- Neuroblastoma PDFDocument5 pagesNeuroblastoma PDFHanna G. FauziaNo ratings yet
- DX N Manage Lower Limb CellulitisDocument4 pagesDX N Manage Lower Limb CellulitisNurul Dwi UtamiNo ratings yet
- GC Damage HC PDFDocument5 pagesGC Damage HC PDFNurul Dwi UtamiNo ratings yet
- Guidelines IDSA STI 2014Document43 pagesGuidelines IDSA STI 2014Nurul Dwi UtamiNo ratings yet
- A 16 Suppl1 029Document11 pagesA 16 Suppl1 029Nurul Dwi UtamiNo ratings yet
- Brain Mapping On EA St36 by FmriDocument4 pagesBrain Mapping On EA St36 by FmriNurul Dwi Utami100% (1)
- Ea Prvents Cognitive Deficit in Pilocarpine Induced RatDocument5 pagesEa Prvents Cognitive Deficit in Pilocarpine Induced RatNurul Dwi UtamiNo ratings yet
- Community Building ProcessDocument17 pagesCommunity Building ProcessKarolina HutagalungNo ratings yet
- Self-motivation quiz tipsDocument1 pageSelf-motivation quiz tipsRose D GuzmanNo ratings yet
- Model of Decision MakingDocument34 pagesModel of Decision MakingPalalikesjujubesNo ratings yet
- Complete Guide To Communication Problems After StrokeDocument22 pagesComplete Guide To Communication Problems After Strokeapi-215453798100% (1)
- Treatment of Child Victims of Abuse and NeglectDocument18 pagesTreatment of Child Victims of Abuse and NeglectSri Harsha KothapalliNo ratings yet
- Randomized trial therapy worksheetDocument2 pagesRandomized trial therapy worksheetmermerytaNo ratings yet
- AnemiaDocument40 pagesAnemiaRajaNo ratings yet
- Job Shadowing PresentationDocument8 pagesJob Shadowing Presentationapi-360560383No ratings yet
- ent-CLINICAL CASE REPORTDocument23 pagesent-CLINICAL CASE REPORTAlexandra DukeNo ratings yet
- The Contribution of Carl Rogers and Humanistic Theory To The Understanding of Personality DevelopmentDocument13 pagesThe Contribution of Carl Rogers and Humanistic Theory To The Understanding of Personality DevelopmentOtto_CondliffeNo ratings yet
- Cognitive Behavioral Model of Clinical Perfectionism Shafran Cooper Fairburn 2002 En-UsDocument1 pageCognitive Behavioral Model of Clinical Perfectionism Shafran Cooper Fairburn 2002 En-UsPavlov PicassoNo ratings yet
- Cheat Sheet (AutoRecovered)Document2 pagesCheat Sheet (AutoRecovered)Garry LeeNo ratings yet
- Healthy Hair Guide Magazine PDFDocument15 pagesHealthy Hair Guide Magazine PDFjagan100% (1)
- JVPDocument5 pagesJVPYhr YhNo ratings yet
- KlsjlkdajslkdajslkDocument4 pagesKlsjlkdajslkdajslkRejed VillanuevaNo ratings yet
- YOGA THERAPY for Digestive HealthDocument3 pagesYOGA THERAPY for Digestive Healthrabirm77No ratings yet
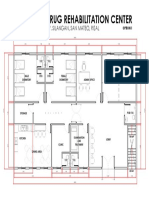
- Proposed Drug Rehabilitation Center: Monterey Sudb., Brgy. Silangan, San Mateo, RizalDocument1 pageProposed Drug Rehabilitation Center: Monterey Sudb., Brgy. Silangan, San Mateo, RizalJonathan MazonNo ratings yet
- Mobility: How To Fix The 3 Most Common Mobility IssuesDocument32 pagesMobility: How To Fix The 3 Most Common Mobility Issuespablo ito100% (4)
- Psychoanalytic EssayDocument7 pagesPsychoanalytic Essayapi-462360394No ratings yet
- Spiramycin Drug Information for Toxoplasmosis TreatmentDocument14 pagesSpiramycin Drug Information for Toxoplasmosis TreatmentRevina AmaliaNo ratings yet
- NeuroblastomaDocument10 pagesNeuroblastomadita100% (1)
- Revised Case Report - HemorrhoidsDocument47 pagesRevised Case Report - Hemorrhoidschristina_love08100% (2)
- SWOT Analysis of The Emergency ServiceDocument20 pagesSWOT Analysis of The Emergency ServiceScribdTranslationsNo ratings yet
- Nursing Care Plan - Acute Pain Assessment Diagnosis Scientific Rationale Planning Intervention Rationale EvaluationDocument3 pagesNursing Care Plan - Acute Pain Assessment Diagnosis Scientific Rationale Planning Intervention Rationale EvaluationNicole cuencosNo ratings yet
- Poisoning and Environmental Exposure PDFDocument148 pagesPoisoning and Environmental Exposure PDFAbdullahNo ratings yet
- Caries Predication, Risk Assessment and Treatment PlanningDocument74 pagesCaries Predication, Risk Assessment and Treatment PlanningmohammadNo ratings yet