You might also like
- Chronic Renal FailureDocument13 pagesChronic Renal FailureAnusha VergheseNo ratings yet
- Pathofishiologis Chronic Kidney DiseaseDocument4 pagesPathofishiologis Chronic Kidney DiseaseNisaNo ratings yet
- Presented By: Sonia Dagar: Renal FailureDocument40 pagesPresented By: Sonia Dagar: Renal FailureRavanshi ThakurNo ratings yet
- Renal FailureDocument33 pagesRenal FailureDeniela Jamaicy Herbert100% (6)
- Renal FailureDocument3 pagesRenal Failurerjones53No ratings yet
- Renal Failure: Prepare by Mohammed Sahman Basees Alsharari - 391110030Document33 pagesRenal Failure: Prepare by Mohammed Sahman Basees Alsharari - 391110030jsksNo ratings yet
- Renal SystemDocument20 pagesRenal SystemRahul DasNo ratings yet
- Kidney Function and Chronic Renal FailureDocument50 pagesKidney Function and Chronic Renal FailureKevin MontoyaNo ratings yet
- Renal FailureDocument4 pagesRenal FailureMunish DograNo ratings yet
- CKD NotesDocument11 pagesCKD NotesMaria WibawaNo ratings yet
- CaseStudy ChronicRenalFailureDocument29 pagesCaseStudy ChronicRenalFailureCarlcedrick ManlapusNo ratings yet
- Renal Failure: Prepare by Mohammed Sahman Basees Alsharari - 391110030Document31 pagesRenal Failure: Prepare by Mohammed Sahman Basees Alsharari - 391110030jsksNo ratings yet
- Pathophysiology ESRDDocument9 pagesPathophysiology ESRDJaye DangoNo ratings yet
- Acute Renal Failure TeoriDocument24 pagesAcute Renal Failure TeoriVera Andri YaniNo ratings yet
- Pathophysiology CKDDocument3 pagesPathophysiology CKDCyndi Jane Bandin CruzataNo ratings yet
- crf03 1Document16 pagescrf03 1Aswin DamodaranNo ratings yet
- FLG 332 Renal Physiology-3 (2019)Document29 pagesFLG 332 Renal Physiology-3 (2019)Huzaifa KhanNo ratings yet
- Renal Failure Renal Failure Renal Failure: Causes and ManagementDocument13 pagesRenal Failure Renal Failure Renal Failure: Causes and Managementjaycey24RM,RNNo ratings yet
- Kidney FailureDocument2 pagesKidney Failuredanee しNo ratings yet
- KidneyDocument18 pagesKidneyRacha MougharbelNo ratings yet
- Chronic Kidney DiseaseDocument17 pagesChronic Kidney Diseaseniken_rizkiNo ratings yet
- Renal Failur E: Mamta Kumari Asst - Prof. Igims-ConDocument51 pagesRenal Failur E: Mamta Kumari Asst - Prof. Igims-ConMamta KumariNo ratings yet
- Chronic Kidney DiseaseDocument41 pagesChronic Kidney DiseaseveraveroNo ratings yet
- NephritisDocument16 pagesNephritisyikesNo ratings yet
- Acute Renal FailureDocument4 pagesAcute Renal FailurePerrilyn PereyNo ratings yet
- Laporan Pendahuluan Gagal Ginjal KronikDocument26 pagesLaporan Pendahuluan Gagal Ginjal Kronikarief rafsanjaniNo ratings yet
- Acute Kidney Failure OverviewDocument13 pagesAcute Kidney Failure Overviewsingireddi1revathiNo ratings yet
- Acute-Renal-Failure Lecture OnlyDocument17 pagesAcute-Renal-Failure Lecture OnlyeyesontheskyNo ratings yet
- BubreDocument10 pagesBubreharryNo ratings yet
- Heart Failure Is Common and Is Due To Sodium and Water Retention, Acid-BaseDocument3 pagesHeart Failure Is Common and Is Due To Sodium and Water Retention, Acid-BaseLuna AstanehNo ratings yet
- Acute Renal Failure Nursing CareDocument85 pagesAcute Renal Failure Nursing Careellise abundoNo ratings yet
- Acute and Chronic Renal FailureDocument21 pagesAcute and Chronic Renal FailureStephina ImmaculateNo ratings yet
- Chronic Renal FailureDocument28 pagesChronic Renal FailuremarshmalouNo ratings yet
- Acute Renal Failur E: By: Miss Santoshi Naik Assistant Professor Yenepoya Pharmacy College & Research CentreDocument15 pagesAcute Renal Failur E: By: Miss Santoshi Naik Assistant Professor Yenepoya Pharmacy College & Research CentreAnusikta PandaNo ratings yet
- AlaaDocument7 pagesAlaaduskblade502No ratings yet
- Your Kidneys: Anatomy, Function and Common ConditionsDocument2 pagesYour Kidneys: Anatomy, Function and Common ConditionsEarl Jay UayanNo ratings yet
- Askep Gagal Ginjal - Ns. FitrioDocument32 pagesAskep Gagal Ginjal - Ns. FitriodesyNo ratings yet
- Renal Failure Cronic Group 6Document18 pagesRenal Failure Cronic Group 6Wiwi Hardiyanti100% (1)
- Acute Renal FailureDocument9 pagesAcute Renal FailureNipul MondolNo ratings yet
- Chronic Kidney Disease OverviewDocument28 pagesChronic Kidney Disease Overviewomie22100% (9)
- Chronic Kidney DiseaseDocument8 pagesChronic Kidney DiseaseAyiessa_AJNo ratings yet
- Case Analysis FinDocument64 pagesCase Analysis Finlhiamdm1208No ratings yet
- Lecture 3 CKDDocument53 pagesLecture 3 CKDPharmswipe KenyaNo ratings yet
- Renal Physiology StagesDocument22 pagesRenal Physiology Stagesسمية صالحNo ratings yet
- Acute Renal Failure & Chronic Renal FailureDocument38 pagesAcute Renal Failure & Chronic Renal FailureArti GondNo ratings yet
- Renal FailuireDocument39 pagesRenal FailuireAmbroseNo ratings yet
- Renal Diseaseppt2789Document112 pagesRenal Diseaseppt2789Sundeep SharmaNo ratings yet
- Chronic Renal FailureDocument4 pagesChronic Renal FailureHercy Emarie AnabeNo ratings yet
- Etiology: I. Predisposing FactorDocument12 pagesEtiology: I. Predisposing FactorIbcp SalvacionNo ratings yet
- HTTPDocument10 pagesHTTPkasmiatiNo ratings yet
- Presentation مسنين عمليDocument19 pagesPresentation مسنين عمليzoubia209No ratings yet
- Chronic Kidney Disease - Genitourinary Disorders - MSD Manual Professional EditionDocument11 pagesChronic Kidney Disease - Genitourinary Disorders - MSD Manual Professional EditionAdi PomeranzNo ratings yet
- Chronic Kidney DiseaseDocument11 pagesChronic Kidney DiseaseMah AlfaroNo ratings yet
- Manage Renal Failure Through Prevention, Treatment and Self-CareDocument13 pagesManage Renal Failure Through Prevention, Treatment and Self-CaretrrdsNo ratings yet
- LP CKD AnemiaDocument12 pagesLP CKD AnemiaNanan SaputraNo ratings yet
- Chronic Kidney Failure Transplant 2Document22 pagesChronic Kidney Failure Transplant 2Gail Leslie HernandezNo ratings yet
- Acute Kidney InjuryDocument6 pagesAcute Kidney Injurytherese BNo ratings yet
- The Renal Diet Kitchen: 60+ Quick and Delicious Renal Diet Recipes to Improve Kidney FunctionFrom EverandThe Renal Diet Kitchen: 60+ Quick and Delicious Renal Diet Recipes to Improve Kidney FunctionNo ratings yet
- Summary of GradesDocument1 pageSummary of GradesVecky TolentinoNo ratings yet
- What Is End-Stage Renal Disease (ESRD) ?Document2 pagesWhat Is End-Stage Renal Disease (ESRD) ?Vecky TolentinoNo ratings yet
- Day 5 Time Activities Specific Activities Staff Nurses: College of NursingDocument2 pagesDay 5 Time Activities Specific Activities Staff Nurses: College of NursingVecky TolentinoNo ratings yet
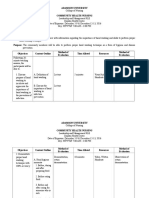
- Management Plan: Head Nurse: Tolentino, Ericka Louise Area: FEU-NRMFDocument2 pagesManagement Plan: Head Nurse: Tolentino, Ericka Louise Area: FEU-NRMFVecky TolentinoNo ratings yet
- ESRD Lab Test, Drug Study and NCPDocument3 pagesESRD Lab Test, Drug Study and NCPVecky TolentinoNo ratings yet
- ESRDDocument37 pagesESRDVecky TolentinoNo ratings yet
- ESRDDocument37 pagesESRDVecky TolentinoNo ratings yet
- Pathophy EsrdDocument4 pagesPathophy EsrdVecky TolentinoNo ratings yet
- ESRD Lab Test, Drug Study and NCPDocument3 pagesESRD Lab Test, Drug Study and NCPVecky TolentinoNo ratings yet
- Teaching Plan Hand WashingDocument4 pagesTeaching Plan Hand WashingVecky Tolentino50% (2)
- FliersDocument2 pagesFliersVecky TolentinoNo ratings yet
- Nursing Care for FatigueDocument2 pagesNursing Care for FatigueVecky TolentinoNo ratings yet
- Discharge Plan Post SeizureDocument2 pagesDischarge Plan Post SeizureVecky TolentinoNo ratings yet
- Case Study Colon CancerDocument8 pagesCase Study Colon CancerVecky Tolentino100% (4)
- Nursing Care for FatigueDocument2 pagesNursing Care for FatigueVecky TolentinoNo ratings yet
- FliersDocument2 pagesFliersVecky TolentinoNo ratings yet
- Drug StudyDocument41 pagesDrug StudyVecky TolentinoNo ratings yet
- Viii. Nursing Care Plan Assessment Nursing Diagnosis Planning Interventions Rationale EvaluationDocument6 pagesViii. Nursing Care Plan Assessment Nursing Diagnosis Planning Interventions Rationale EvaluationVecky TolentinoNo ratings yet
- Case Study Post Stroke SeizuresDocument12 pagesCase Study Post Stroke SeizuresVecky TolentinoNo ratings yet