You might also like
- Cancer Regional Therapy: HAI, HIPEC, HILP, ILI, PIPAC and BeyondFrom EverandCancer Regional Therapy: HAI, HIPEC, HILP, ILI, PIPAC and BeyondNo ratings yet
- Rectal Cancer: International Perspectives on Multimodality ManagementFrom EverandRectal Cancer: International Perspectives on Multimodality ManagementBrian G. CzitoNo ratings yet
- CA ServiksDocument10 pagesCA ServiksAndi Farid ANo ratings yet
- NPCDocument8 pagesNPCArsy Mira PertiwiNo ratings yet
- Neoadjuvant chemoradiotherapy followed by surgery standard for esophageal cancerDocument14 pagesNeoadjuvant chemoradiotherapy followed by surgery standard for esophageal cancerkrsna2studyNo ratings yet
- MeduloblastomaDocument7 pagesMeduloblastomasilvia erfanNo ratings yet
- 2021 Consolidation Theraphy in Esophageal CancerDocument6 pages2021 Consolidation Theraphy in Esophageal CancerykommNo ratings yet
- Nej Me 068121Document2 pagesNej Me 068121anissakikinNo ratings yet
- Carboplatin-Paclitaxel vs Carboplatin-Pegylated Liposomal Doxorubicin for Platinum-Sensitive Ovarian CancerDocument6 pagesCarboplatin-Paclitaxel vs Carboplatin-Pegylated Liposomal Doxorubicin for Platinum-Sensitive Ovarian Cancerbettzy21No ratings yet
- Referatneoadjuvan EnggrisDocument22 pagesReferatneoadjuvan EnggrisPonco RossoNo ratings yet
- Adjuvant Systemic Therapies in Breast CancerDocument19 pagesAdjuvant Systemic Therapies in Breast CancerSapp ChaamaraNo ratings yet
- Allen2021 Article ChemotherapyVersusChemotherapyDocument8 pagesAllen2021 Article ChemotherapyVersusChemotherapyXavier QuinteroNo ratings yet
- Magic TrailDocument10 pagesMagic Trailchootu509No ratings yet
- Glockzin - 2012 - Surgical Oncology Clinics of North AmericaDocument9 pagesGlockzin - 2012 - Surgical Oncology Clinics of North AmericaPraveen RavishankaranNo ratings yet
- Breast-Cancer Adjuvant Therapy With Zoledronic Acid: Methods Study PatientsDocument11 pagesBreast-Cancer Adjuvant Therapy With Zoledronic Acid: Methods Study PatientsAn'umillah Arini ZidnaNo ratings yet
- CDDP Gemzar BilcanDocument9 pagesCDDP Gemzar BilcanhodimirekNo ratings yet
- Analysis of Compliance, Toxicity and Survival WeeklyDocument11 pagesAnalysis of Compliance, Toxicity and Survival Weeklydanu20No ratings yet
- Curran 2011Document9 pagesCurran 2011Nguyễn Hoàng PhúcNo ratings yet
- Cancer Colo-Rectal StudiuDocument3 pagesCancer Colo-Rectal StudiuEghet SilviuNo ratings yet
- 013 - Surgeon-Led-Clinical-Trials-in-Pancrea - 2023 - Surgical-Oncology-Clinics-of-NorDocument9 pages013 - Surgeon-Led-Clinical-Trials-in-Pancrea - 2023 - Surgical-Oncology-Clinics-of-NorDr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- Capecitabine Monotherapy For Recurrent and Metastatic Nasopharyngeal CancerDocument6 pagesCapecitabine Monotherapy For Recurrent and Metastatic Nasopharyngeal Cancertrifamonika23No ratings yet
- Standard surgical procedures and adjuvant therapies for colon cancerDocument46 pagesStandard surgical procedures and adjuvant therapies for colon cancerNadia Iriana DewiNo ratings yet
- Intergroup 0123Document8 pagesIntergroup 0123radonc17No ratings yet
- Resection of The Primary Colorectal CancDocument7 pagesResection of The Primary Colorectal CancjorgehogNo ratings yet
- Bristow 2002Document12 pagesBristow 2002Lưu Chính HữuNo ratings yet
- 1 4918218693336367165 PDFDocument14 pages1 4918218693336367165 PDFjorgeaznarNo ratings yet
- The OncologistDocument7 pagesThe OncologistManunart FeungpeanNo ratings yet
- Preoperative and Adjuvant Therapies For Upper Gastrointestinal CancersDocument7 pagesPreoperative and Adjuvant Therapies For Upper Gastrointestinal Cancersajaymanvikar007No ratings yet
- Clinical Impact of External Radiotherapy in Non-Metastatic Esophageal Cancer According To Histopathological SubtypeDocument12 pagesClinical Impact of External Radiotherapy in Non-Metastatic Esophageal Cancer According To Histopathological SubtypesilviailieNo ratings yet
- TraztuzumabDocument8 pagesTraztuzumabArlina Wiyata GamaNo ratings yet
- Updates in Management of Ampullary Carcinomas: Highlight ArticleDocument4 pagesUpdates in Management of Ampullary Carcinomas: Highlight Articlecorinna291No ratings yet
- Brief CommunicationDocument13 pagesBrief CommunicationsantovazNo ratings yet
- JCOG9912Document7 pagesJCOG9912BobQuNo ratings yet
- P ('t':'3', 'I':'176969959') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Document8 pagesP ('t':'3', 'I':'176969959') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Cecep Saeful HudaNo ratings yet
- The Comparison of Surgery and Chemo-Radio Therapy in Locally Recurrent Colorectal CancerDocument4 pagesThe Comparison of Surgery and Chemo-Radio Therapy in Locally Recurrent Colorectal CancerInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- AsdasdDocument10 pagesAsdasdAdhi PratamaNo ratings yet
- Short-Term Metronidazole Not Linked To CancerDocument1 pageShort-Term Metronidazole Not Linked To CancerTika Ayu andaniNo ratings yet
- Pancreatic Cancer Literature ReviewDocument10 pagesPancreatic Cancer Literature Reviewea813c29No ratings yet
- HCC 5Document7 pagesHCC 5TeodoraNo ratings yet
- 1475 2891 12 118Document8 pages1475 2891 12 118SunardiasihNo ratings yet
- Bladder Cancer LancetDocument11 pagesBladder Cancer LancetYesenia HuertaNo ratings yet
- Adjuvant Versus Salvage Radiotherapy Following Radical Prostatectomy: Do The AUA/ASTRO Guidelines Have All The Answers?Document6 pagesAdjuvant Versus Salvage Radiotherapy Following Radical Prostatectomy: Do The AUA/ASTRO Guidelines Have All The Answers?Anonymous jBoDXi3sNo ratings yet
- Axtner Et Al. - 2016 - Health Services Research of Integrative Oncology in Palliative Care of Patients With Advanced Pancreatic CancerDocument10 pagesAxtner Et Al. - 2016 - Health Services Research of Integrative Oncology in Palliative Care of Patients With Advanced Pancreatic CancerMaría Reynel TarazonaNo ratings yet
- 009 - The-Perioperative-and-Operative-Management-of - 2023 - Surgical-Oncology-ClinicsDocument17 pages009 - The-Perioperative-and-Operative-Management-of - 2023 - Surgical-Oncology-ClinicsDr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- The Optimal Neoadjuvant Treatment of Locally Advanced Esophageal CancerDocument11 pagesThe Optimal Neoadjuvant Treatment of Locally Advanced Esophageal CancerdjonesthoracicNo ratings yet
- Effect of More Vs Less Frequent Follow-Up Testing On Overall and Colorectal Cancer-Specific Mortality in Patients With Stage II or III Colorectal CancerDocument9 pagesEffect of More Vs Less Frequent Follow-Up Testing On Overall and Colorectal Cancer-Specific Mortality in Patients With Stage II or III Colorectal CancerMr. LNo ratings yet
- Evidence-Based Guidance For Breast Cancer SurvivorshipDocument19 pagesEvidence-Based Guidance For Breast Cancer SurvivorshipZuriNo ratings yet
- 211 FullDocument17 pages211 Fullalfarisi_auliaNo ratings yet
- Eficacia de Azul de Metileno VO en ColonoDocument11 pagesEficacia de Azul de Metileno VO en ColonoMarielaDiazNo ratings yet
- Treatment of Metastatic Endometrial CancerDocument24 pagesTreatment of Metastatic Endometrial CancerKaroline Pascoal Ilidio PeruchiNo ratings yet
- Ournal of Linical Ncology: OriginalDocument10 pagesOurnal of Linical Ncology: OriginalMaulida Nurazmi OctaviaNo ratings yet
- Pathological complete response in recurrent colon cancer following neoadjuvant radiotherapy and intraperitoneal chemotherapyDocument4 pagesPathological complete response in recurrent colon cancer following neoadjuvant radiotherapy and intraperitoneal chemotherapyAlice AugustinNo ratings yet
- JCO 2003 Lin 631 7Document7 pagesJCO 2003 Lin 631 7Adhika Manggala DharmaNo ratings yet
- Research Article: Prevalence of Cachexia in Cancer PatientsDocument9 pagesResearch Article: Prevalence of Cachexia in Cancer Patientsadri20121989No ratings yet
- Neoadjuvant Paclitaxel For Operable Breast Cancer: Multicenter Phase II Trial With Clinical OutcomesDocument6 pagesNeoadjuvant Paclitaxel For Operable Breast Cancer: Multicenter Phase II Trial With Clinical OutcomesSubhash SugathanNo ratings yet
- Jurnal DMDocument10 pagesJurnal DMMalisa LukmanNo ratings yet
- Esofago Carvical Valmasoni 2018Document9 pagesEsofago Carvical Valmasoni 2018Carlos N. Rojas PuyolNo ratings yet
- Prognostic Factors in Nasopharyngeal Carcinoma With Synchronous Liver Metastasis: A Retrospective Study For The Management of TreatmentDocument7 pagesPrognostic Factors in Nasopharyngeal Carcinoma With Synchronous Liver Metastasis: A Retrospective Study For The Management of TreatmentChairul Nurdin AzaliNo ratings yet
- Sequential Chemoradiotherapy With Gemcitabine and Cisplatin For Locoregionally Advanced Nasopharyngeal CarcinomaDocument9 pagesSequential Chemoradiotherapy With Gemcitabine and Cisplatin For Locoregionally Advanced Nasopharyngeal CarcinomadheaonyonNo ratings yet
- Cytotoxic Treatment of Metastatic Breast Cancer Which Drugs and Drug Combinations To UseDocument7 pagesCytotoxic Treatment of Metastatic Breast Cancer Which Drugs and Drug Combinations To UseGamer MadaNo ratings yet
- A Population-Based Cohort Study On Adherence To Practice Guidelines For Adjuvant Chemotherapy in Colorectal CancerDocument9 pagesA Population-Based Cohort Study On Adherence To Practice Guidelines For Adjuvant Chemotherapy in Colorectal CancerFatona AgungNo ratings yet
- Soal Penilaian Tengah Semester XIDocument1 pageSoal Penilaian Tengah Semester XIFatona AgungNo ratings yet
- Puskesmas Solo Free Health Care Clinic Patient Visit Recap February 2019Document294 pagesPuskesmas Solo Free Health Care Clinic Patient Visit Recap February 2019Fatona AgungNo ratings yet
- Clinico-Pathological Correlation of SerialDocument5 pagesClinico-Pathological Correlation of SerialFatona AgungNo ratings yet
- Glioblastoma5 PDFDocument10 pagesGlioblastoma5 PDFFatona AgungNo ratings yet
- Glioblastoma3 PDFDocument29 pagesGlioblastoma3 PDFFatona AgungNo ratings yet
- Glioblastoma4 PDFDocument29 pagesGlioblastoma4 PDFFatona AgungNo ratings yet
- GlioblastomaDocument11 pagesGlioblastomaFatona AgungNo ratings yet
- Lampiran PetaDocument4 pagesLampiran PetaFatona AgungNo ratings yet
- Little Child Dry Your Crying EyesDocument1 pageLittle Child Dry Your Crying EyesFatona AgungNo ratings yet
- SxceoeoeoDocument6 pagesSxceoeoeolionfairwayNo ratings yet
- Almost EasyDocument1 pageAlmost EasyFatona AgungNo ratings yet
- Little Child Dry Your Crying EyesDocument1 pageLittle Child Dry Your Crying EyesFatona AgungNo ratings yet
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Review More Than BlueDocument1 pageReview More Than BlueB2 - Dimatulac, Jessieryl A.No ratings yet
- GlutathioneDocument21 pagesGlutathioneGB R100% (1)
- ISSA Senior Fitness Certification Chapter PreviewDocument21 pagesISSA Senior Fitness Certification Chapter Previewscorpion9990% (1)
- Kuretase Case Report 2Document3 pagesKuretase Case Report 2Lydia AmaliaNo ratings yet
- 2.High-Resolution CT of The Lung EDITIA A-3-A.Document736 pages2.High-Resolution CT of The Lung EDITIA A-3-A.RamonataleNo ratings yet
- OSU Orthopaedics Accomplishments Report 2010Document32 pagesOSU Orthopaedics Accomplishments Report 2010osuorthopaedicsNo ratings yet
- Angela Tang-Tan ResumeDocument2 pagesAngela Tang-Tan Resumeapi-459113948No ratings yet
- Intravenous PyelogramDocument23 pagesIntravenous Pyelogramrachael100% (1)
- Gastrointestinal Bleeding Guide: Causes, Symptoms, Diagnosis & TreatmentDocument46 pagesGastrointestinal Bleeding Guide: Causes, Symptoms, Diagnosis & TreatmentSyarifah FauziahNo ratings yet
- Food Adultration ObjectiveDocument11 pagesFood Adultration ObjectiveGourav Som0% (1)
- 2015 PM Lecture 4 Barium EnemaDocument62 pages2015 PM Lecture 4 Barium EnemaObrian ReidNo ratings yet
- Preventing Breast Cancer Through Lifestyle and ScreeningDocument5 pagesPreventing Breast Cancer Through Lifestyle and ScreeningDana LebadaNo ratings yet
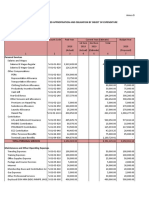
- Programmed Appropriation and Obligation by Object of ExpenditureDocument7 pagesProgrammed Appropriation and Obligation by Object of ExpenditureKristin Villaseñor-MercadoNo ratings yet
- Akupuntur InfertilityDocument7 pagesAkupuntur Infertilitybustanul aswatNo ratings yet
- Tobacco Smoking-Associated Alterations in The Immune Microenvironment of Squamous Cell CarcinomasDocument7 pagesTobacco Smoking-Associated Alterations in The Immune Microenvironment of Squamous Cell CarcinomasKamado NezukoNo ratings yet
- Gestational Trophoblastic DiseaseDocument40 pagesGestational Trophoblastic DiseaseAayupta Mohanty100% (2)
- Autoimmune EncephalitisDocument9 pagesAutoimmune EncephalitisDini Fajriah OmariNo ratings yet
- Genetic Attribution For Schizophrenia, Depression, and Skin Cancer: Impact On Social DistanceDocument7 pagesGenetic Attribution For Schizophrenia, Depression, and Skin Cancer: Impact On Social DistancenigoNo ratings yet
- Pre TestDocument6 pagesPre TestPRINTDESK by DanNo ratings yet
- Gastrointestinal Endoscopy Volume 71 Issue 7 2010 (Doi 10.1016/j.gie.2009.12.029) Lisette G. Capelle Annemarie C. de Vries Jelle Haringsma Fran - The Staging of Gastritis With The OLGA System by PDFDocument9 pagesGastrointestinal Endoscopy Volume 71 Issue 7 2010 (Doi 10.1016/j.gie.2009.12.029) Lisette G. Capelle Annemarie C. de Vries Jelle Haringsma Fran - The Staging of Gastritis With The OLGA System by PDFAleida VivalloNo ratings yet
- Annals of Medicine - HPV VaccineDocument12 pagesAnnals of Medicine - HPV VaccineJudicial Watch, Inc.100% (3)
- 006 Pathology MCQ ACEM Primary CellularDocument5 pages006 Pathology MCQ ACEM Primary CellularIrum RafeeqNo ratings yet
- GI Disorders NursingDocument93 pagesGI Disorders NursingAmy100% (4)
- Guide: DR Srinath Rao Presenter:Dr SR Soumya (Materia Medica MD Part-1) 15/12/14Document50 pagesGuide: DR Srinath Rao Presenter:Dr SR Soumya (Materia Medica MD Part-1) 15/12/14Krishna Veni100% (2)
- Colour BlindnessDocument4 pagesColour BlindnessDanial HazimNo ratings yet
- Kerala Uiversity Bhms PapersDocument31 pagesKerala Uiversity Bhms PapersKarthikNo ratings yet
- Ayva Içerik Cydonia Oblonga PDFDocument20 pagesAyva Içerik Cydonia Oblonga PDFZeynep Emirhan ŞenyüzNo ratings yet
- Follicular Cholecystitis With Cholelithiasis A Rare Case ReportDocument3 pagesFollicular Cholecystitis With Cholelithiasis A Rare Case ReportSSR-IIJLS JournalNo ratings yet
- Clinical Summary Guide 05Document2 pagesClinical Summary Guide 05Diarti_PMIKNo ratings yet
- CeramFab Inc. & WYG Refractories SuitDocument27 pagesCeramFab Inc. & WYG Refractories SuitBenjamin DuerNo ratings yet