You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Test Bank Contemporary Behavior Therapy - Michael-Spiegler - 6th EditionDocument12 pagesTest Bank Contemporary Behavior Therapy - Michael-Spiegler - 6th Editionlewisbacha0% (1)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Fixed-Bed Platforming General Operating Manual Rev 6 PDFDocument512 pagesFixed-Bed Platforming General Operating Manual Rev 6 PDFaditya surya tama100% (4)
- Ib Items: PotionsDocument8 pagesIb Items: PotionsZeNoWTFNo ratings yet
- Manual NSD70D EnglishDocument155 pagesManual NSD70D Englishnarvis1No ratings yet
- Marine Pollution Bulletin: Sivanandham Vignesh, Krishnan Muthukumar, Rathinam Arthur JamesDocument11 pagesMarine Pollution Bulletin: Sivanandham Vignesh, Krishnan Muthukumar, Rathinam Arthur JamesGeorgiana-LuizaNo ratings yet
- Chapter 2 ManojDocument4 pagesChapter 2 ManojBro FistoNo ratings yet
- Multiple Bank Accounts Registration FormDocument2 pagesMultiple Bank Accounts Registration FormAjith JainNo ratings yet
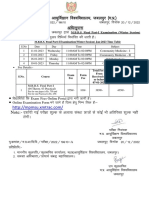
- MBBS Final Part-I (Winter Session) Time Table (Jan 2023)Document1 pageMBBS Final Part-I (Winter Session) Time Table (Jan 2023)crystal mindNo ratings yet
- Cottonhill - Red Collection PDFDocument33 pagesCottonhill - Red Collection PDFVioricaNo ratings yet
- Using Casts For ImmobilizationDocument17 pagesUsing Casts For Immobilizationmpmayer2No ratings yet
- Pidato Bahasa InggrisDocument4 pagesPidato Bahasa InggrisAriya Manikmaya100% (1)
- Chapter 1 EconomicsDocument5 pagesChapter 1 Economicsjordan cedeñoNo ratings yet
- Household Chemical Poisoning GuideDocument9 pagesHousehold Chemical Poisoning GuideAshley DayagNo ratings yet
- Medray Letterhead TemplateDocument5 pagesMedray Letterhead TemplateSteve NjugiNo ratings yet
- Palm Avenue ApartmentsDocument6 pagesPalm Avenue Apartmentsassistant_sccNo ratings yet
- Face SerumDocument10 pagesFace SerumLiliana CojocaruNo ratings yet
- Shell Alexia 40 cylinder oil designed for IMO 2020 complianceDocument2 pagesShell Alexia 40 cylinder oil designed for IMO 2020 complianceStefas DimitriosNo ratings yet
- Mini-Pitch Session Exceptionalities and InclusionDocument18 pagesMini-Pitch Session Exceptionalities and Inclusionapi-486583325No ratings yet
- TDDDocument4 pagesTDDJay VibhaniNo ratings yet
- Deped Memo No. 165, S 2010: WastedDocument6 pagesDeped Memo No. 165, S 2010: WastedJayne InoferioNo ratings yet
- Waste Management: Spoilage of LandscapeDocument7 pagesWaste Management: Spoilage of Landscapeshauryasahu2004No ratings yet
- Sohail KhanDocument3 pagesSohail KhanRashid Muhammad SarwarNo ratings yet
- 29 TM5 Kireina Akhlak AnnisaDocument30 pages29 TM5 Kireina Akhlak AnnisaTamaraNo ratings yet
- Courses at NeevDocument10 pagesCourses at NeevDr Mohan SavadeNo ratings yet
- LENZE E84AVxCx - 8400 StateLine-HighLine-TopLine 0.25-45kW - v9-0 - ENDocument291 pagesLENZE E84AVxCx - 8400 StateLine-HighLine-TopLine 0.25-45kW - v9-0 - ENClaudioNo ratings yet
- Is411 8Document1 pageIs411 8amoghimiNo ratings yet
- C11984569 Signed OfferLetterDocument10 pagesC11984569 Signed OfferLetterSiriNo ratings yet
- Aloe Vera as an Alternative Treatment for Wound HealingDocument5 pagesAloe Vera as an Alternative Treatment for Wound HealingJeffllanoNo ratings yet
- Physiology of Women Reproduction SystemDocument52 pagesPhysiology of Women Reproduction Systemram kumarNo ratings yet
- Cooking - Sauces and Marinade RecipesDocument96 pagesCooking - Sauces and Marinade Recipesagape_1st7100% (3)