You might also like
- 2021 Physician Compensation Report - Updated 0821Document24 pages2021 Physician Compensation Report - Updated 0821Michael Knapp100% (3)
- Money Tooth BookDocument41 pagesMoney Tooth BookVizi Adrian0% (2)
- InLine PoM Edition GruebelDocument28 pagesInLine PoM Edition GruebelFabio WenoNo ratings yet
- Louis Hardan Mobile Dental Photography Part I ViaDocument9 pagesLouis Hardan Mobile Dental Photography Part I ViaMuchlis Fauzi ENo ratings yet
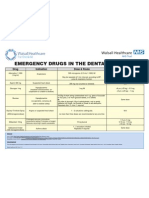
- Emergency Drugs Poster - Layout 1 in Dental PracticeDocument1 pageEmergency Drugs Poster - Layout 1 in Dental PracticeFady AtefNo ratings yet
- Endo Vs Implant SeminarDocument25 pagesEndo Vs Implant Seminarsweetminu99100% (1)
- Fixed Orthodontic Appliances: A Practical GuideFrom EverandFixed Orthodontic Appliances: A Practical GuideRating: 1 out of 5 stars1/5 (1)
- Nursing Care of A Family With An InfantDocument26 pagesNursing Care of A Family With An InfantJc GarciaNo ratings yet
- Increased Vertical Dimension of Occlusion Signs Symptoms Diagnosis Treatment and OptionsDocument6 pagesIncreased Vertical Dimension of Occlusion Signs Symptoms Diagnosis Treatment and OptionsJericho MedionNo ratings yet
- Impacted Wisdom Tooth, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandImpacted Wisdom Tooth, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Receding Gums, (Gingival Recession) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandReceding Gums, (Gingival Recession) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
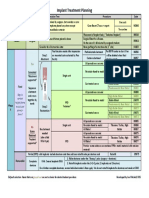
- Implant TX Plan GridDocument1 pageImplant TX Plan GridAhmed BadrNo ratings yet
- Decision Tree For Oral Mucosal Lesion PDFDocument1 pageDecision Tree For Oral Mucosal Lesion PDFcreature123100% (1)
- 10 Must Know Factors of OcclusionDocument2 pages10 Must Know Factors of OcclusionGreg Sitek0% (1)
- Cracked Tooth PresentationDocument36 pagesCracked Tooth Presentationmirfanulhaq100% (1)
- Spear Anterior Open BitesDocument28 pagesSpear Anterior Open BitesMahmoud AlsuleimanNo ratings yet
- Space Regaining PedoDocument39 pagesSpace Regaining PedoFourthMolar.comNo ratings yet
- Guidelines On Dental Record KeepingDocument8 pagesGuidelines On Dental Record KeepingXubair AhmedNo ratings yet
- A Critical Appraisal of Tongue-Thrusting-Tulley PDFDocument11 pagesA Critical Appraisal of Tongue-Thrusting-Tulley PDFmalifaragNo ratings yet
- Cross BiteDocument32 pagesCross Bitestgdc100% (1)
- Discovering The Artist Inside A Three-Step Approach To Predictable Aesthetic Smile Designs, Part 1Document13 pagesDiscovering The Artist Inside A Three-Step Approach To Predictable Aesthetic Smile Designs, Part 1ilich sevillaNo ratings yet
- Ortho NotesDocument71 pagesOrtho NotesJames Deguzman100% (1)
- PATIENT EVALUATION Complete Denture JDDocument40 pagesPATIENT EVALUATION Complete Denture JDjen100% (1)
- The Course of TimeDocument9 pagesThe Course of TimeMoroianu MariusNo ratings yet
- Articaine Dental Update 2015Document5 pagesArticaine Dental Update 2015Ashley WrightNo ratings yet
- Pickard's Manual-Tooth Wear (Dragged)Document8 pagesPickard's Manual-Tooth Wear (Dragged)Adit MehtaNo ratings yet
- Prolonged Retention, Ankylosis and Infraocclusion of Deciduous Teeth Ok OkDocument5 pagesProlonged Retention, Ankylosis and Infraocclusion of Deciduous Teeth Ok OkRahulLife'sNo ratings yet
- Why Dentistry Fails The 10 Must Know Factors of Occlusion The Dawson Academy 2021 WhitepaperDocument3 pagesWhy Dentistry Fails The 10 Must Know Factors of Occlusion The Dawson Academy 2021 WhitepaperManuel CastilloNo ratings yet
- Philosophy of Orthodontic 1Document54 pagesPhilosophy of Orthodontic 1Angie Sona Putri NonegrinaNo ratings yet
- Management of Impacted CanineDocument97 pagesManagement of Impacted CanineOluseye SoyeboNo ratings yet
- Biomechanics of BioprogressiveDocument31 pagesBiomechanics of BioprogressiveMinh ĐạtNo ratings yet
- Designing Successful Removable PartialDenturesDocument9 pagesDesigning Successful Removable PartialDenturesHatem AbouelnasrNo ratings yet
- J Esthet Restor Dent - 2020 - Vargas - A Systematic Approach To Contouring and Polishing Anterior Resin CompositeDocument7 pagesJ Esthet Restor Dent - 2020 - Vargas - A Systematic Approach To Contouring and Polishing Anterior Resin CompositeScarleth Stephania Perez CastilloNo ratings yet
- Breakfast Fo Ods Satiety: Mary Ellen Camire & Megan BlackmoreDocument6 pagesBreakfast Fo Ods Satiety: Mary Ellen Camire & Megan BlackmoreDavid Dragoş100% (1)
- Anterior Open BiteDocument7 pagesAnterior Open BiteGowriNo ratings yet
- The Prosthodontic Management of Endodontically Treated Teeth - A Literature Review. Part I. SuccesDocument8 pagesThe Prosthodontic Management of Endodontically Treated Teeth - A Literature Review. Part I. SucceskochikaghochiNo ratings yet
- Dental OsteologyDocument154 pagesDental OsteologyfabrizioaryanNo ratings yet
- "Introduction To Biomimetic Dentistry": How To Get Bonded & Stay BondedDocument2 pages"Introduction To Biomimetic Dentistry": How To Get Bonded & Stay BondedJuan Augusto Fernández TarazonaNo ratings yet
- Space Maintenance: Emma Laing, Paul Ashley, Farhad B. Naini & Daljit S. GillDocument8 pagesSpace Maintenance: Emma Laing, Paul Ashley, Farhad B. Naini & Daljit S. GillAnonymous JR1VNCNo ratings yet
- Veneer Series PT 1Document6 pagesVeneer Series PT 1Cornelia Gabriela OnuțNo ratings yet
- Smile Line and Periodontium Visibility: Clinical and Research ReportDocument9 pagesSmile Line and Periodontium Visibility: Clinical and Research ReportMed-Amine TouloutNo ratings yet
- Guidelines BookDocument16 pagesGuidelines BookAdel ElaroudNo ratings yet
- Traumatic Injuries To The Teeth4541Document114 pagesTraumatic Injuries To The Teeth4541Irfan AliNo ratings yet
- A Beginners Guide To Lateral Cephalometric RadiographsDocument4 pagesA Beginners Guide To Lateral Cephalometric RadiographsClaudiaNo ratings yet
- 4 Bad Habits ODocument10 pages4 Bad Habits OPurnama SyahbaniNo ratings yet
- A Clinical Guide To Occlusion An IntroductionDocument75 pagesA Clinical Guide To Occlusion An IntroductionAndrei Oana100% (1)
- Open Drainage or NotDocument6 pagesOpen Drainage or Notjesuscomingsoon2005_No ratings yet
- Esthetic RPDDocument7 pagesEsthetic RPDapi-3710948100% (1)
- Restorative Management of The Worn Dentition Pt1Document6 pagesRestorative Management of The Worn Dentition Pt1Sherif ReffatNo ratings yet
- Kois DSDocument12 pagesKois DSanees jamalNo ratings yet
- Periodontal Assessment and Managment in Fixed ProsthodonticsDocument56 pagesPeriodontal Assessment and Managment in Fixed ProsthodonticsCristina Ene100% (2)
- Flap Design For Minor Oral SurgeryDocument22 pagesFlap Design For Minor Oral SurgerysevattapillaiNo ratings yet
- The Truth About OcclusionDocument37 pagesThe Truth About Occlusiondrsmriti100% (2)
- Hall TechniqueDocument19 pagesHall TechniqueanatomimanusiaNo ratings yet
- Working Length DeterminationDocument97 pagesWorking Length Determinationrolly_jatinNo ratings yet
- Fudamentals of Biomechanics and Biomechanics of Levelling and Aligning Includes Biomechanics of Molar Control PDFDocument326 pagesFudamentals of Biomechanics and Biomechanics of Levelling and Aligning Includes Biomechanics of Molar Control PDFVioleta PajicNo ratings yet
- MRI Scanning and OrthodonticsDocument7 pagesMRI Scanning and OrthodonticsAmit SagarNo ratings yet
- Functional Occlusion and The Mounting of The CastsDocument88 pagesFunctional Occlusion and The Mounting of The CastsAina SalsaNo ratings yet
- A Restrospective Periodontal Assessment of 137 Teeth After Featheredge Preparation and GingittageDocument11 pagesA Restrospective Periodontal Assessment of 137 Teeth After Featheredge Preparation and GingittageBelen AntoniaNo ratings yet
- Ejed 9 3 Tirlet p354Document16 pagesEjed 9 3 Tirlet p354Ángela María GuevaraNo ratings yet
- 31 SJ BDJ 2014 953Document7 pages31 SJ BDJ 2014 953Juan Augusto Fernández TarazonaNo ratings yet
- 1 TelescopicDocument9 pages1 TelescopicAdmen PasaribuNo ratings yet
- Composite Resins ReviewDocument6 pagesComposite Resins ReviewDavid ColonNo ratings yet
- 7491 PDFDocument10 pages7491 PDFMuchlis Fauzi ENo ratings yet
- Functional Biomimetic Dental Restoration PDFDocument30 pagesFunctional Biomimetic Dental Restoration PDFMuchlis Fauzi ENo ratings yet
- Schwartz-Carabelli JHE PDFDocument20 pagesSchwartz-Carabelli JHE PDFMuchlis Fauzi ENo ratings yet
- Composite Resins ReviewDocument6 pagesComposite Resins ReviewDavid ColonNo ratings yet
- Gendent So16 OwensDocument7 pagesGendent So16 OwensMuchlis Fauzi ENo ratings yet
- Simpleandaethetictreatmentforanteriortoothwear PDFDocument5 pagesSimpleandaethetictreatmentforanteriortoothwear PDFMuchlis Fauzi ENo ratings yet
- Closure of Midline Diastema by Direct Composite Resin Build-Up Using A Customized Matrix Technique - A Case ReportDocument4 pagesClosure of Midline Diastema by Direct Composite Resin Build-Up Using A Customized Matrix Technique - A Case ReportMuchlis Fauzi ENo ratings yet
- 1143 1412842796 PDFDocument3 pages1143 1412842796 PDFMuchlis Fauzi ENo ratings yet
- 1143 1412842796 PDFDocument3 pages1143 1412842796 PDFMuchlis Fauzi ENo ratings yet
- Indirect Pulp CappingDocument5 pagesIndirect Pulp CappingNaji Z. ArandiNo ratings yet
- Treze Anos de Acompanhamento Clínico de Restaurações Conservativas de Resina Composta No Fechamento de Diastemas AnterioresDocument5 pagesTreze Anos de Acompanhamento Clínico de Restaurações Conservativas de Resina Composta No Fechamento de Diastemas AnterioresMuchlis Fauzi ENo ratings yet
- CPS Feb14 Utilizing Innovative Matrix Systems WCE 4 0Document5 pagesCPS Feb14 Utilizing Innovative Matrix Systems WCE 4 0Muchlis Fauzi ENo ratings yet
- Print Hitam Putih 1Document15 pagesPrint Hitam Putih 1Muchlis Fauzi ENo ratings yet
- GuttaCore - Brochure 2017 Rev2 - ENDocument7 pagesGuttaCore - Brochure 2017 Rev2 - ENMuchlis Fauzi ENo ratings yet
- A Conservative Approach in Restoration With Combination Fixed Partial Denture: Case ReportDocument4 pagesA Conservative Approach in Restoration With Combination Fixed Partial Denture: Case ReportMuchlis Fauzi ENo ratings yet
- B.A.,D.D.S.,M.S.D. : Herbert Werdlow, Bethesda, MDDocument7 pagesB.A.,D.D.S.,M.S.D. : Herbert Werdlow, Bethesda, MDMuchlis Fauzi ENo ratings yet
- E676 PDFDocument6 pagesE676 PDFMuchlis Fauzi ENo ratings yet
- Neutral Zone Concept and TechniqueDocument6 pagesNeutral Zone Concept and TechniqueJasween KaurNo ratings yet
- Gangguan Psychophysiologic Sebagai Salah Satu Penyebab Kelainan Pada Sendi TemporomandibulaDocument44 pagesGangguan Psychophysiologic Sebagai Salah Satu Penyebab Kelainan Pada Sendi TemporomandibulaAnggita Maharani PutriNo ratings yet
- 2016 Article 171Document9 pages2016 Article 171Muchlis Fauzi ENo ratings yet
- 10 1111@j 1365-2842 2012 02304 XDocument11 pages10 1111@j 1365-2842 2012 02304 XMuchlis Fauzi ENo ratings yet
- 2.endo PerioLesionPartIITheTreatmentDocument8 pages2.endo PerioLesionPartIITheTreatmentMuchlis Fauzi ENo ratings yet
- Biological and Clinical Rationale For Vital Pulp TherapyDocument10 pagesBiological and Clinical Rationale For Vital Pulp TherapyMuchlis Fauzi ENo ratings yet
- G PulpDocument9 pagesG PulpwindhaNo ratings yet
- Apd MGZ p3-1-1Document15 pagesApd MGZ p3-1-1Muchlis Fauzi ENo ratings yet
- z350xt TPPDocument36 pagesz350xt TPPPutri MortezaNo ratings yet
- Bro TCforSikaCarboDurStructuralStrengtheningSystems UsDocument11 pagesBro TCforSikaCarboDurStructuralStrengtheningSystems UsMuchlis Fauzi ENo ratings yet
- Manual GISDocument36 pagesManual GISDanil Pangestu ChandraNo ratings yet
- 2014 EN AdvancedBootkitTechniquesOnAndroid ChenZhangqiShendiDocument66 pages2014 EN AdvancedBootkitTechniquesOnAndroid ChenZhangqiShendihombre pocilgaNo ratings yet
- Make Swiss RollDocument16 pagesMake Swiss RollFelicia LiNo ratings yet
- Yume Beauty Price ListDocument1 pageYume Beauty Price ListjessicaelaNo ratings yet
- Teoria Do Campo Ligante - Part IIDocument25 pagesTeoria Do Campo Ligante - Part IIArthurGrafdeSousaNo ratings yet
- Location: Map of Naga CityDocument2 pagesLocation: Map of Naga Citycatherine boragayNo ratings yet
- X FEDEX EIDocument13 pagesX FEDEX EINISREEN WAYANo ratings yet
- Critique PaperDocument1 pageCritique PapernicolealerNo ratings yet
- Allnex Powder BrochureDocument28 pagesAllnex Powder BrochureandreathomeNo ratings yet
- Ragin Cajun PDFDocument2 pagesRagin Cajun PDFjosemfcNo ratings yet
- Rubric On Baking CakesDocument3 pagesRubric On Baking CakesshraddhaNo ratings yet
- Normal Microflora of Human BodyDocument14 pagesNormal Microflora of Human BodySarah PavuNo ratings yet
- JEE Mains 2024 Question Paper Shift 2 27 JanDocument4 pagesJEE Mains 2024 Question Paper Shift 2 27 JanAnjali SahooNo ratings yet
- 6L45, 6L50, 6L80, 6L90: Time Tested - Industry TrustedDocument1 page6L45, 6L50, 6L80, 6L90: Time Tested - Industry TrustedCelso BidinotiNo ratings yet
- Remote Control RC902V1 ManualDocument3 pagesRemote Control RC902V1 ManualdezdoNo ratings yet
- Nitrile Butadiene Rubber (NBR), Synthetic Latex: ApplicationDocument2 pagesNitrile Butadiene Rubber (NBR), Synthetic Latex: ApplicationbobNo ratings yet
- Paracetamol DegradationDocument9 pagesParacetamol DegradationTruyền Phạm MinhNo ratings yet
- MCQDocument5 pagesMCQJagdishVankar100% (1)
- Recipe Booklet PRINT VERSIONDocument40 pagesRecipe Booklet PRINT VERSIONjtsunami815100% (1)
- Efficiency Improvement Oppertunities With BLDC Fan PDFDocument14 pagesEfficiency Improvement Oppertunities With BLDC Fan PDFjust_4_u_dear_in9549No ratings yet
- 8291 w13 Ms 22Document8 pages8291 w13 Ms 22Caterina De LucaNo ratings yet
- Health and Illness Answer-8Document2 pagesHealth and Illness Answer-8June DumdumayaNo ratings yet
- Tiling Checklist UpdatedDocument3 pagesTiling Checklist UpdatedSayed Taimoor shahNo ratings yet
- Moody's Financial Metrics 2007Document35 pagesMoody's Financial Metrics 2007Adrian IlieNo ratings yet
- Polymer ProDocument25 pagesPolymer ProJeerisuda KingklangNo ratings yet
- Raymond Lo - The Feng Shui of Swine FluDocument1 pageRaymond Lo - The Feng Shui of Swine Fluay2004jan100% (1)
- Nuclear Over Hauser Enhancement (NOE)Document18 pagesNuclear Over Hauser Enhancement (NOE)Fatima AhmedNo ratings yet
- Vishaka GuidelinesDocument4 pagesVishaka GuidelinesAakashKumarNo ratings yet