You might also like
- Stemi Acute Coronary Syndrome: Dr. Muh A Sungkar, SPPD, SPJP, KKVDocument35 pagesStemi Acute Coronary Syndrome: Dr. Muh A Sungkar, SPPD, SPJP, KKVCoass BonamNo ratings yet
- Kegawatan Jantung - MeDocument41 pagesKegawatan Jantung - MeNam Min BinNo ratings yet
- Chronic Inflammatory Demyelinating PolyneuropathyDocument7 pagesChronic Inflammatory Demyelinating PolyneuropathyApriliaNo ratings yet
- Immunopatologi Sepsis - DR Nur Farhanah SPPD K-PTIDocument29 pagesImmunopatologi Sepsis - DR Nur Farhanah SPPD K-PTIanita tri hastutiNo ratings yet
- MateriDocument39 pagesMateriDR BASUKINo ratings yet
- Cardiovascular in Elderly NewDocument23 pagesCardiovascular in Elderly NewVania OktavianiNo ratings yet
- Penatalaksanaan DSSDocument29 pagesPenatalaksanaan DSSTugas HeinzNo ratings yet
- Flail Chest 2Document16 pagesFlail Chest 2talithanrNo ratings yet
- Testicular Torsion: Journal ReadingDocument14 pagesTesticular Torsion: Journal ReadingRizkiYudaPurnomoNo ratings yet
- Gasem MH HANTA Salatiga 2019Document43 pagesGasem MH HANTA Salatiga 2019ChristianNo ratings yet
- Fecal Incontinence Treatment & ManagementDocument11 pagesFecal Incontinence Treatment & ManagementParijatak AurvedaNo ratings yet
- Ecg Crit - CareDocument55 pagesEcg Crit - CarekrismatactayNo ratings yet
- Flail Chest: DR Okagbue IzuchukwuDocument21 pagesFlail Chest: DR Okagbue IzuchukwuOkagbue IzuchukwuNo ratings yet
- Cardiac Dysfunction in Neurocritical Care.Document14 pagesCardiac Dysfunction in Neurocritical Care.Angela Moreira ArteagaNo ratings yet
- ICBA NotesDocument60 pagesICBA NotesAndrew EldeiryNo ratings yet
- SS II.1.1 Update On Typhoid Management - Dr. Adityo Susilo, SpPD-KPTI PDFDocument34 pagesSS II.1.1 Update On Typhoid Management - Dr. Adityo Susilo, SpPD-KPTI PDFWisnu Yudho HNo ratings yet
- Acute Promyelocytic Leukemia Part-1Document8 pagesAcute Promyelocytic Leukemia Part-1Francisco Ignacio Reiser ValverdeNo ratings yet
- Chronic Inflammatory Demyelinating PolyradiculoneuropathyDocument12 pagesChronic Inflammatory Demyelinating Polyradiculoneuropathyrafael rocha novaesNo ratings yet
- Diagnosis and Management of Idiopathic Normal-Pressure HydrocephalusDocument11 pagesDiagnosis and Management of Idiopathic Normal-Pressure HydrocephalusPablo Sousa Casasnovas100% (1)
- Sinus Rhythm and Sinus and Atrial DysrhythmiasDocument41 pagesSinus Rhythm and Sinus and Atrial Dysrhythmiasclaudia brongNo ratings yet
- HFpEF MeDocument28 pagesHFpEF MeRidwan YasinNo ratings yet
- Assessment and Initial Management Trauma PatientDocument69 pagesAssessment and Initial Management Trauma PatientdrpagrawNo ratings yet
- Axis DeviationDocument26 pagesAxis DeviationDanial HassanNo ratings yet
- Cardiovascular Nursing: Study Online atDocument7 pagesCardiovascular Nursing: Study Online atLilly DayeNo ratings yet
- Varices Esophagus PDFDocument7 pagesVarices Esophagus PDFDimas ErlanggaNo ratings yet
- Heparin and WarfarinDocument2 pagesHeparin and WarfarinBaeyer100% (1)
- Preanesthesia Evaluation For Noncardiac Surgery - UpToDate PDFDocument86 pagesPreanesthesia Evaluation For Noncardiac Surgery - UpToDate PDFCharlie Bellow100% (1)
- CardiologyDocument62 pagesCardiologysee yinNo ratings yet
- BMAT-Bedside Mobility Assessment Tool: by Amber Perez ADN, BSB, CSPHPDocument36 pagesBMAT-Bedside Mobility Assessment Tool: by Amber Perez ADN, BSB, CSPHPConvalescent Nursing HomeNo ratings yet
- Buku CHFDocument59 pagesBuku CHFSylvia PertiwiNo ratings yet
- Fluids and Electrolytes Lesson Outline For BBDocument14 pagesFluids and Electrolytes Lesson Outline For BBdlneisha61100% (1)
- Job Description of A Nurse AnesthetistDocument3 pagesJob Description of A Nurse AnesthetistlhalamNo ratings yet
- Catheter Directed Thrombolysis: Gan Dunnington M.D. Stanford Vascular Conference 9/12/05Document25 pagesCatheter Directed Thrombolysis: Gan Dunnington M.D. Stanford Vascular Conference 9/12/05Pratik SahaNo ratings yet
- Valvular Heart DiseaseDocument41 pagesValvular Heart DiseaseVirendra Shekhawat100% (1)
- Valvular Heart Disease: Bekele T. (MD)Document47 pagesValvular Heart Disease: Bekele T. (MD)alehegn beleteNo ratings yet
- Surgery Study GuideDocument27 pagesSurgery Study GuideNatalie100% (1)
- Surgical Intervention in Management of Heart Failure: DR Royman Simanjuntak Sp. BTKVDocument118 pagesSurgical Intervention in Management of Heart Failure: DR Royman Simanjuntak Sp. BTKVEmily RumiaNo ratings yet
- Valvular Heart Disease: Presented by DR Mirjana Milutinovic Professor, SJSMDocument69 pagesValvular Heart Disease: Presented by DR Mirjana Milutinovic Professor, SJSMAbanoub AwadallaNo ratings yet
- Valvular Heart DiseaseDocument10 pagesValvular Heart DiseaseEzyan SyaminNo ratings yet
- Aortic Stenosis: EtiologiesDocument16 pagesAortic Stenosis: Etiologiesneutrophil0329No ratings yet
- CVS ReviewDocument61 pagesCVS Reviewafaq alismailiNo ratings yet
- Shock, Arrest, Syncope PhysiopathologyDocument54 pagesShock, Arrest, Syncope PhysiopathologyParsa EbrahimpourNo ratings yet
- Surgery Study GuideDocument27 pagesSurgery Study GuideMaryNguyenNo ratings yet
- Penyakit Katup Jantung: Dr. Tjatur Winarsanto SPPD Rs CiremaiDocument59 pagesPenyakit Katup Jantung: Dr. Tjatur Winarsanto SPPD Rs CiremaianisamayaNo ratings yet
- Cardiogenic ShockDocument189 pagesCardiogenic ShockDian PuspaNo ratings yet
- Pathology of Cardiovascular SystemDocument75 pagesPathology of Cardiovascular Systemefri100% (2)
- Heart Valve DiseaseDocument67 pagesHeart Valve DiseaseSaba SivaNo ratings yet
- Angelina A Joho MSC in Critical Care and TraumaDocument50 pagesAngelina A Joho MSC in Critical Care and TraumaZabron LuhendeNo ratings yet
- Rheumatic Heart DiseaseDocument47 pagesRheumatic Heart DiseaseGideon K. MutaiNo ratings yet
- Cvs-k7-Valvular Heart Disease Nora2010Document52 pagesCvs-k7-Valvular Heart Disease Nora2010shiloinNo ratings yet
- Evar Osana - Nysana.finalDocument47 pagesEvar Osana - Nysana.finalStefanSteinNo ratings yet
- Department of Internal Medicine III Aortic Stenosis: - Rajkumar Subasaravanan Subgroup "12"Document51 pagesDepartment of Internal Medicine III Aortic Stenosis: - Rajkumar Subasaravanan Subgroup "12"Suba Saravanan 12No ratings yet
- Ischemic Heart Disease: Dr. Pearl Myers Path Fall 2011 With Acknowledgement To DR SADocument67 pagesIschemic Heart Disease: Dr. Pearl Myers Path Fall 2011 With Acknowledgement To DR SADylan KremerNo ratings yet
- UMS20 Medical 20 Short 20 and 20 Long 20 Cases 20 Record 20 Second 20 EditiDocument132 pagesUMS20 Medical 20 Short 20 and 20 Long 20 Cases 20 Record 20 Second 20 EditiUchiha AnzarNo ratings yet
- Aortic Stenosis AmendillaDocument31 pagesAortic Stenosis AmendillaVadim BursacovschiNo ratings yet
- Aortic Valve SurgeryDocument73 pagesAortic Valve SurgeryRezwanul Hoque Bulbul100% (2)
- Aortic Stenosis: General ConsiderationsDocument5 pagesAortic Stenosis: General ConsiderationsShe DearNo ratings yet
- Ischemic Heart DiseaseDocument67 pagesIschemic Heart Diseasealfaz lakhani80% (5)
- Nursing Acn-IiDocument80 pagesNursing Acn-IiMunawar100% (6)
- Mechanical Complications of AMI-1Document33 pagesMechanical Complications of AMI-1Matthew BanksNo ratings yet
- Bagi '2016 Antibiotic - Blood Brain Barrier - PPT'Document31 pagesBagi '2016 Antibiotic - Blood Brain Barrier - PPT'RidhaNo ratings yet
- Anatomi Faring Dan Laring (Dr. Yani)Document18 pagesAnatomi Faring Dan Laring (Dr. Yani)Maylinda PutriNo ratings yet
- Analisis Probit-Modul MPDocument11 pagesAnalisis Probit-Modul MPRidhaNo ratings yet
- Data SimulasiDocument8 pagesData SimulasiRidhaNo ratings yet
- Peripheral Nerve DisordersDocument66 pagesPeripheral Nerve DisordersReno Andri0% (1)
- Assisted Reproduction Technology Dr. MeidonaDocument85 pagesAssisted Reproduction Technology Dr. Meidonanadya sahnazNo ratings yet
- Virus: The Legend ImmortalDocument19 pagesVirus: The Legend ImmortalRidhaNo ratings yet
- Overview Sistem SarafDocument45 pagesOverview Sistem SarafRidhaNo ratings yet
- Neuroimaging Kelainan Vertebra (Dr. Bekti)Document46 pagesNeuroimaging Kelainan Vertebra (Dr. Bekti)Nafi24No ratings yet
- Endang - Berfikir Sebagai Kegiatan Seorang MuslimDocument8 pagesEndang - Berfikir Sebagai Kegiatan Seorang MuslimRevi A. NindivtiraNo ratings yet
- Farmakologi Analgetik NSAID (Dr. Atina)Document56 pagesFarmakologi Analgetik NSAID (Dr. Atina)RidhaNo ratings yet
- Lezione 7. Immunita - MucosaleDocument86 pagesLezione 7. Immunita - MucosaleRidhaNo ratings yet
- Peripheral Nerve DisordersDocument53 pagesPeripheral Nerve DisordersRidhaNo ratings yet
- DengueDocument33 pagesDengueRidhaNo ratings yet
- Keganasan ParuDocument19 pagesKeganasan ParuRidhaNo ratings yet
- Endang - Berfikir Sebagai Kegiatan Seorang MuslimDocument8 pagesEndang - Berfikir Sebagai Kegiatan Seorang MuslimRevi A. NindivtiraNo ratings yet
- PHNDocument34 pagesPHNRidhaNo ratings yet
- EB4 GutDevelopmentDocument33 pagesEB4 GutDevelopmentRidhaNo ratings yet
- Diabetic Foot InfectionDocument26 pagesDiabetic Foot InfectionAmanda Abdat100% (1)
- Billirubin MetabolismDocument10 pagesBillirubin MetabolismAnantyo Ari SaputroNo ratings yet
- Kuliah Vena Cava SindromeDocument24 pagesKuliah Vena Cava SindromeRidhaNo ratings yet
- AtelactasisDocument89 pagesAtelactasiswahyuNo ratings yet
- AtelactasisDocument89 pagesAtelactasiswahyuNo ratings yet
- Fisiologi Hati Dan Kandung EmpeduDocument42 pagesFisiologi Hati Dan Kandung EmpeduRidhaNo ratings yet
- Energy Metabolism in MuscleDocument19 pagesEnergy Metabolism in MuscleRidhaNo ratings yet
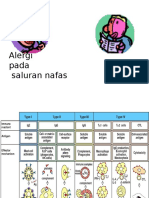
- Alergi NafasDocument18 pagesAlergi NafasRidhaNo ratings yet
- Drugs in Respiratory SystemDocument120 pagesDrugs in Respiratory SystemRidhaNo ratings yet
- Coagulase Test Intended UseDocument1 pageCoagulase Test Intended UseRidhaNo ratings yet
- Alergi NafasDocument18 pagesAlergi NafasRidhaNo ratings yet
- Hemolysis - Blood Agar Intended UseDocument1 pageHemolysis - Blood Agar Intended UseRidhaNo ratings yet
- Etp fOR Dasda PDFDocument6 pagesEtp fOR Dasda PDFDesignNo ratings yet
- UNSAFE aCTS & UNSAFECONDITIONDocument48 pagesUNSAFE aCTS & UNSAFECONDITIONSn CarbonelNo ratings yet
- Gallstone, Choledocholithiasis, Ascending CholangistisDocument12 pagesGallstone, Choledocholithiasis, Ascending CholangistisNurulasyikin MAA100% (1)
- Advantage CP File - FinalDocument254 pagesAdvantage CP File - FinalvegSpamNo ratings yet
- A Solution-Focused Approach To Rational-Emotive Behavior Therapy - Toward A Theoretical IntegrationDocument22 pagesA Solution-Focused Approach To Rational-Emotive Behavior Therapy - Toward A Theoretical Integrationsolutions4familyNo ratings yet
- Health 10: 3 Quarter Week 7Document10 pagesHealth 10: 3 Quarter Week 7Maria Rose Tariga Aquino50% (2)
- Introduction To Epidemiology: The Basic Science of Public HealthDocument34 pagesIntroduction To Epidemiology: The Basic Science of Public Healthapi-19641337100% (1)
- Ramsay Sedation Scale and How To Use ItDocument10 pagesRamsay Sedation Scale and How To Use ItAdinda Putra PradhanaNo ratings yet
- H. Pylori IgA ELISA Package InsertDocument2 pagesH. Pylori IgA ELISA Package Inserttalha saleemNo ratings yet
- Wu 2008Document8 pagesWu 2008SergioNo ratings yet
- Varma Practictioner GuideDocument9 pagesVarma Practictioner GuideGoutham PillaiNo ratings yet
- Catalogo Baby MarketDocument53 pagesCatalogo Baby Marketmiguel quispeNo ratings yet
- Brazilian Sanitary Guide For Cruise ShipsDocument82 pagesBrazilian Sanitary Guide For Cruise ShipsStanislav KozhuharovNo ratings yet
- Social Work MaterialDocument214 pagesSocial Work MaterialBala Tvn100% (2)
- Lifestyle Related Diseases HandoutsDocument1 pageLifestyle Related Diseases HandoutsJonathan RagadiNo ratings yet
- Group 2 - Up-Fa1-Stem11-19 - Chapter IiDocument7 pagesGroup 2 - Up-Fa1-Stem11-19 - Chapter IijamesrusselNo ratings yet
- Fetal Mummification in CowsDocument22 pagesFetal Mummification in CowsTahseen AlamNo ratings yet
- Usmart 3200T Plus BrochureDocument4 pagesUsmart 3200T Plus BrochureMNo ratings yet
- Homoeopathic Drug Proving: Randomised Double Blind Placebo Controlled TrialDocument9 pagesHomoeopathic Drug Proving: Randomised Double Blind Placebo Controlled TrialParag SharmaNo ratings yet
- Engl7 Q4 W4 Determining-Accuracy Villanueva Bgo Reviewed-1Document18 pagesEngl7 Q4 W4 Determining-Accuracy Villanueva Bgo Reviewed-1johbaguilatNo ratings yet
- Tumors of Head and Neck RegionDocument94 pagesTumors of Head and Neck Regionpoornima vNo ratings yet
- AishwaryaDocument52 pagesAishwaryamohitNo ratings yet
- World AIDS Day - December 1, 2019 Status of HIV Case-Based Surveillance Implementation - 39 U.S. PEPFAR-Supported Countries, May-July 2019Document16 pagesWorld AIDS Day - December 1, 2019 Status of HIV Case-Based Surveillance Implementation - 39 U.S. PEPFAR-Supported Countries, May-July 2019worksheetbookNo ratings yet
- Chapter 020Document59 pagesChapter 020api-263755297No ratings yet
- Experimental and Clinical Reconstructive Microsurgery 1st Ed. 2003 EditionDocument559 pagesExperimental and Clinical Reconstructive Microsurgery 1st Ed. 2003 EditionLuka DamjanovicNo ratings yet
- Basic Education For Autistic Children Using Interactive Video GamesDocument5 pagesBasic Education For Autistic Children Using Interactive Video GamesEwerton DuarteNo ratings yet
- Good Knight 420 GPatien ManualDocument30 pagesGood Knight 420 GPatien ManualJose Antonio AlcazarNo ratings yet
- Causas de Pancitopenia Canina y FelinaDocument12 pagesCausas de Pancitopenia Canina y FelinaMarisol AsakuraNo ratings yet
- Transferring A Dependent Patient From Bed To ChairDocument5 pagesTransferring A Dependent Patient From Bed To Chairapi-26570979No ratings yet
- Estimation of Blood GlucoseDocument3 pagesEstimation of Blood Glucosepodcast gazalNo ratings yet