You might also like
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Physiotherapy Management of Tennis Elbow................ ArticleDocument5 pagesPhysiotherapy Management of Tennis Elbow................ ArticleRupika SodhiNo ratings yet
- Postural DeviationsDocument40 pagesPostural DeviationsMohamed Tariq Acchha100% (2)
- Length Tension Testing Book 1, Lower Quadrant: A Workbook of Manual Therapy TechniquesFrom EverandLength Tension Testing Book 1, Lower Quadrant: A Workbook of Manual Therapy TechniquesRating: 3.5 out of 5 stars3.5/5 (3)
- Prolapsed Intervertebral DiscDocument14 pagesProlapsed Intervertebral DiscMartin Sage100% (1)
- Length Tension Testing Book 2, Upper Quadrant: A Workbook of Manual Therapy TechniquesFrom EverandLength Tension Testing Book 2, Upper Quadrant: A Workbook of Manual Therapy TechniquesRating: 1 out of 5 stars1/5 (1)
- 1990 Pekoz Design of Cold-Formed Steel Screw ConnectionsDocument15 pages1990 Pekoz Design of Cold-Formed Steel Screw ConnectionsmabuhamdNo ratings yet
- Quarter 2-Module 7 Social and Political Stratification: Department of Education Republic of The PhilippinesDocument21 pagesQuarter 2-Module 7 Social and Political Stratification: Department of Education Republic of The Philippinestricia100% (5)
- Joint Capsular PatternsDocument4 pagesJoint Capsular Patternsherlitaandri annisaNo ratings yet
- GaitDocument85 pagesGaitOmar Midani100% (1)
- PsychFirstAidSchools PDFDocument186 pagesPsychFirstAidSchools PDFAna ChicasNo ratings yet
- Biomechanics of Knee - 1Document43 pagesBiomechanics of Knee - 1mahiNo ratings yet
- (Durt, - Christoph - Fuchs, - Thomas - Tewes, - Christian) Embodiment, Enaction, and Culture PDFDocument451 pages(Durt, - Christoph - Fuchs, - Thomas - Tewes, - Christian) Embodiment, Enaction, and Culture PDFnlf2205100% (3)
- Coaches Manual 2011Document168 pagesCoaches Manual 2011avist80100% (1)
- Biomechanics of SpineDocument22 pagesBiomechanics of Spineyuvraj100% (1)
- Intoduction To MaitlandDocument25 pagesIntoduction To MaitlandAsad Chaudhary100% (1)
- Coxa VaraDocument19 pagesCoxa VaraFarrukh ShahzadNo ratings yet
- Pes Cavus: Eka Anggraini Padma Vidya GayatriDocument13 pagesPes Cavus: Eka Anggraini Padma Vidya GayatriPadma VidyaNo ratings yet
- Pathomechanics of Knee JointDocument5 pagesPathomechanics of Knee JointWasemBhat100% (3)
- Spinal StabilizationDocument32 pagesSpinal StabilizationLakshita PrajapatiNo ratings yet
- Eugène Burnouf: Legends of Indian Buddhism (1911)Document136 pagesEugène Burnouf: Legends of Indian Buddhism (1911)Levente Bakos100% (1)
- Bio Mechanics of Elbow ComplexDocument11 pagesBio Mechanics of Elbow ComplexMatthew Pugliese50% (2)
- Marketing Plan For Paraiso Islet ResortDocument25 pagesMarketing Plan For Paraiso Islet ResortEllaine Claire Lor100% (1)
- Complications of Bed Rest 1Document4 pagesComplications of Bed Rest 1Geetha Bhavani100% (2)
- Suspension TherapyDocument52 pagesSuspension TherapyROJA MACHERLA0% (1)
- Shweta Aggarwal - Physiotherapy in Musculoskeletal ConditionsDocument283 pagesShweta Aggarwal - Physiotherapy in Musculoskeletal Conditionssaurav.das2030100% (1)
- Biomechanics of Cervical SpineDocument25 pagesBiomechanics of Cervical SpineNithya NithyaNo ratings yet
- Types of Movement &, ExerciseDocument23 pagesTypes of Movement &, ExerciseAhmed50% (2)
- Physiotherapy in General Surgical ConditionDocument7 pagesPhysiotherapy in General Surgical Conditionprofpt98100% (8)
- MPT Books ListDocument3 pagesMPT Books ListImran KhanNo ratings yet
- Neurological Physiotherapy Evaluation Form Wm-2Document15 pagesNeurological Physiotherapy Evaluation Form Wm-2Mohamed HarithNo ratings yet
- Cyriax ConceptDocument26 pagesCyriax ConceptMeenakshiputraeashwarprasad MacherlaNo ratings yet
- Exercises for Patella (Kneecap) Pain, Patellar Tendinitis, and Common Operations for Kneecap Problems: - Understanding kneecap problems and patellar tendinitis - Conservative rehabilitation protocols - Rehabilitation protocols for lateral release, patellar realignment, medial patellofemoral ligament reFrom EverandExercises for Patella (Kneecap) Pain, Patellar Tendinitis, and Common Operations for Kneecap Problems: - Understanding kneecap problems and patellar tendinitis - Conservative rehabilitation protocols - Rehabilitation protocols for lateral release, patellar realignment, medial patellofemoral ligament reRating: 5 out of 5 stars5/5 (1)
- Traumatic Brain Injury Physiotherapy AssessmentDocument20 pagesTraumatic Brain Injury Physiotherapy AssessmentNithin Nair100% (1)
- Physiotherapy in Abdominal SurgeryDocument32 pagesPhysiotherapy in Abdominal SurgeryHUZAIFA YAMAANNo ratings yet
- Physiotherapy For PoliomyelitisDocument16 pagesPhysiotherapy For Poliomyelitisabdalsucs100% (1)
- Physiotherapy For Vascular PatientDocument44 pagesPhysiotherapy For Vascular PatientHaengbokaeyo Hua Min100% (4)
- Role of Physiotherapy in Management of Burns-HshDocument25 pagesRole of Physiotherapy in Management of Burns-HshChristopher Chibueze Igbo100% (1)
- Articular NeurologyDocument14 pagesArticular Neurologykinj100% (1)
- Elementary SurveyingDocument19 pagesElementary SurveyingJefferson EscobidoNo ratings yet
- Erb's PalsyDocument18 pagesErb's PalsyMegha PataniNo ratings yet
- Arif Dirlik - The Origins of Chinese Communism-Oxford University Press, USA (1989)Document335 pagesArif Dirlik - The Origins of Chinese Communism-Oxford University Press, USA (1989)Denisa FeisalNo ratings yet
- Suspension TherapyDocument39 pagesSuspension TherapyFarrukh Shahzad100% (5)
- Supraspinatus TendinitisDocument23 pagesSupraspinatus TendinitisTafzz Sailo0% (1)
- Cyriax - Spine: by DR. Akshay A. Chougule (PT) Orthopaedic Manual TherapistDocument44 pagesCyriax - Spine: by DR. Akshay A. Chougule (PT) Orthopaedic Manual TherapistAishwarya Shah100% (1)
- Peripheral Vascular DiseaseDocument32 pagesPeripheral Vascular DiseaseShy PatelNo ratings yet
- Physiotherapy Management of Vascular DisordersDocument55 pagesPhysiotherapy Management of Vascular DisordersAkheel AhammedNo ratings yet
- Introduction To Manual Therapy Omt (Orthopedic Manual Therapy) Kaltenborn-Evjenth ConceptDocument28 pagesIntroduction To Manual Therapy Omt (Orthopedic Manual Therapy) Kaltenborn-Evjenth ConceptHafsa AzizNo ratings yet
- The Wrist ComplexDocument35 pagesThe Wrist ComplexKeshav Singhmaar AryaNo ratings yet
- Suspension TherapyDocument32 pagesSuspension TherapyNaveen KumarNo ratings yet
- Vertebrobasilar SyndromeDocument14 pagesVertebrobasilar SyndromeHitesh RohitNo ratings yet
- Pinky - Plantar FasciitisDocument34 pagesPinky - Plantar FasciitisRavindra choudharyNo ratings yet
- Myossitis OssificansDocument16 pagesMyossitis OssificansMegha PataniNo ratings yet
- Cervical RibDocument15 pagesCervical RibArko duttaNo ratings yet
- Functional Re-Education TrainingDocument24 pagesFunctional Re-Education Trainingtamilvanan3100% (1)
- Manual Muscle Testing: Grade Value DescriptionDocument40 pagesManual Muscle Testing: Grade Value Descriptionjoanna gurtizaNo ratings yet
- Metatarsalgia: Yakshita Chaube B.P.T Final YearDocument18 pagesMetatarsalgia: Yakshita Chaube B.P.T Final YearKapil LakhwaraNo ratings yet
- Pelvic TiltDocument15 pagesPelvic TiltFarrukh Shahzad80% (5)
- 3 Advantage of Free Ex 3Document13 pages3 Advantage of Free Ex 3Farrukh ShahzadNo ratings yet
- Biomechanics of Wrist ComplexDocument11 pagesBiomechanics of Wrist Complexakheel ahammed100% (2)
- PepDocument8 pagesPepUdayakrishnan P Kanhangad100% (1)
- Causal GiaDocument22 pagesCausal GiaAmitNo ratings yet
- Extension Services and Mobile Health UnitDocument23 pagesExtension Services and Mobile Health UnitKandi IssayaNo ratings yet
- Diabetes and PhysiotherapyDocument15 pagesDiabetes and Physiotherapyane2saNo ratings yet
- DR Vaishali - Therapeutic GymnasiumDocument35 pagesDR Vaishali - Therapeutic Gymnasiumvaishali jagtapNo ratings yet
- Passive Movements PDFDocument18 pagesPassive Movements PDFIndrajith Liyanage100% (8)
- Active and Passive MovementsDocument20 pagesActive and Passive MovementsSajida Bibi Noonari57% (7)
- Biomechanics of Elbow JointDocument10 pagesBiomechanics of Elbow JointGeddam SnehalathaNo ratings yet
- Coughing TechniqueDocument18 pagesCoughing TechniqueSiva ShanmugamNo ratings yet
- GIRDDocument10 pagesGIRDSérgio Xavier SilvaNo ratings yet
- 2010"rehabilitation After Fracture of The Diaphysis of FemurDocument94 pages2010"rehabilitation After Fracture of The Diaphysis of FemurSérgio Xavier SilvaNo ratings yet
- Olympic StudiesDocument380 pagesOlympic StudiesKrist MututanontNo ratings yet
- BIO210 Lab Report 3Document6 pagesBIO210 Lab Report 3Isra MallaNo ratings yet
- Modelling of Short Duration Isopluvial Map For Raichur District KarnatakaDocument4 pagesModelling of Short Duration Isopluvial Map For Raichur District KarnatakaMohammed Badiuddin ParvezNo ratings yet
- SAP CRM Tax ConfigurationDocument18 pagesSAP CRM Tax Configurationtushar_kansaraNo ratings yet
- CBSE Class 12 Business Studies Question Paper 2013 With SolutionsDocument19 pagesCBSE Class 12 Business Studies Question Paper 2013 With SolutionsManormaNo ratings yet
- IUGRDocument4 pagesIUGRMichael Spica RampangileiNo ratings yet
- Full Download Social Animal 14th Edition Aronson Test BankDocument35 pagesFull Download Social Animal 14th Edition Aronson Test Banknaeensiyev100% (32)
- Measures-English, Metric, and Equivalents PDFDocument1 pageMeasures-English, Metric, and Equivalents PDFluz adolfoNo ratings yet
- RPT Form 2 2023Document7 pagesRPT Form 2 2023NOREEN BINTI DOASA KPM-GuruNo ratings yet
- Congental Abdominal Wall DefectsDocument38 pagesCongental Abdominal Wall DefectsAhmad Abu KushNo ratings yet
- Music in The United KingdomDocument33 pagesMusic in The United KingdomIonut PetreNo ratings yet
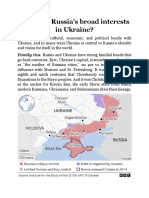
- What Are RussiaDocument3 pagesWhat Are RussiaMuhammad SufyanNo ratings yet
- Aìgas of Bhakti. at The End of The Last Chapter Uddhava Inquired AboutDocument28 pagesAìgas of Bhakti. at The End of The Last Chapter Uddhava Inquired AboutDāmodar DasNo ratings yet
- MISKDocument134 pagesMISKmusyokaNo ratings yet
- Excellent Inverters Operation Manual: We Are Your Excellent ChoiceDocument71 pagesExcellent Inverters Operation Manual: We Are Your Excellent ChoicephaPu4cuNo ratings yet
- Public Administration 2000 - CSS ForumsDocument3 pagesPublic Administration 2000 - CSS ForumsMansoor Ali KhanNo ratings yet
- RF Design MCQ-1Document16 pagesRF Design MCQ-1JeyavelNo ratings yet
- Symbiosis National Aptitude Test (SNAP) 2004: InstructionsDocument21 pagesSymbiosis National Aptitude Test (SNAP) 2004: InstructionsHarsh JainNo ratings yet
- Man Is Made by His BeliefDocument2 pagesMan Is Made by His BeliefLisa KireechevaNo ratings yet
- Spouses Aggabao V. Parulan, Jr. and Parulan G.R. No. 165803, (September 1, 2010) Doctrine (S)Document9 pagesSpouses Aggabao V. Parulan, Jr. and Parulan G.R. No. 165803, (September 1, 2010) Doctrine (S)RJNo ratings yet
- A Global StudyDocument57 pagesA Global StudyRoynal PasaribuNo ratings yet
- Flow ChemistryDocument6 pagesFlow Chemistryrr1819No ratings yet
- Memory and History in The Folklores Reinvented Through BeowulfDocument10 pagesMemory and History in The Folklores Reinvented Through BeowulfDebojyoti DanNo ratings yet