You might also like
- Drug Study (Print3copiesDocument8 pagesDrug Study (Print3copiesPhylum ChordataNo ratings yet
- Nursing Care PlanDocument5 pagesNursing Care PlanNicolne LorraineNo ratings yet
- Drugs Given During Cardiac Arres For CPRDocument5 pagesDrugs Given During Cardiac Arres For CPREevyaj MimiNo ratings yet
- IHDDocument34 pagesIHDElly Msi ProbolinggoNo ratings yet
- Oral Anticoagulants and Antiplatelet Drugs: Treatment With Blood ThinnersDocument8 pagesOral Anticoagulants and Antiplatelet Drugs: Treatment With Blood Thinnershussain AltaherNo ratings yet
- PCI or PTCADocument30 pagesPCI or PTCAMelissa KanggrianiNo ratings yet
- Lesson PlanDocument4 pagesLesson PlanTaylor CarlicNo ratings yet
- Guidelines For The Management of Cardiovascular Diseases in IndiaDocument40 pagesGuidelines For The Management of Cardiovascular Diseases in IndiaViky SinghNo ratings yet
- Cardiac Glycosides 815Document19 pagesCardiac Glycosides 815SanskritiNo ratings yet
- Arterial DisordersDocument40 pagesArterial DisordersSalman KhanNo ratings yet
- Interpreting Pulmonary Function TestsDocument7 pagesInterpreting Pulmonary Function TestsRalucaNo ratings yet
- Angiotensin I Angiotensin II, Angiotensin-Converting Enzyme (ACE) - Vasoconstrictor Angiotensin II Stimulates Aldosterone SecretionDocument11 pagesAngiotensin I Angiotensin II, Angiotensin-Converting Enzyme (ACE) - Vasoconstrictor Angiotensin II Stimulates Aldosterone SecretionAbdullah asadNo ratings yet
- Cataract NotesDocument4 pagesCataract NotesJeremy LauNo ratings yet
- Cardiac BiomarkersDocument10 pagesCardiac BiomarkersfelipetheNo ratings yet
- IHD CAUSES CHEST PAINDocument19 pagesIHD CAUSES CHEST PAINOsama MalikNo ratings yet
- Medication Guide for Alzheimer's PatientsDocument10 pagesMedication Guide for Alzheimer's PatientsBSN 2014No ratings yet
- Emergency Drugs KathDocument29 pagesEmergency Drugs Kathmajin655No ratings yet
- DefibrillationDocument9 pagesDefibrillationJara Maris Moreno BudionganNo ratings yet
- Anaesthesia and Atrial FibrillationDocument15 pagesAnaesthesia and Atrial FibrillationNaresh Dhawan100% (1)
- Cyanotic Congenital Heart DiseasesDocument25 pagesCyanotic Congenital Heart DiseasesAlvin OmondiNo ratings yet
- Respiratory SeminarDocument7 pagesRespiratory SeminarKoochi PoojithaNo ratings yet
- Causes, Symptoms, Pathophysiology and Diagnosis of Atherosclerosis-A ReviewDocument23 pagesCauses, Symptoms, Pathophysiology and Diagnosis of Atherosclerosis-A ReviewBaharudin WahyuNo ratings yet
- Cardiac DefibrillatorsDocument8 pagesCardiac Defibrillatorsصفا طلال نايفNo ratings yet
- Cardio AspirinDocument3 pagesCardio AspirinBayu PrabowoNo ratings yet
- Lower Cholesterol with Atorvastatin (LipitorDocument7 pagesLower Cholesterol with Atorvastatin (LipitorAgronaSlaughterNo ratings yet
- Pro32 SupraventricularTachycardiaDocument1 pagePro32 SupraventricularTachycardiaRonald KendallNo ratings yet
- Adrenergic DrugsDocument33 pagesAdrenergic DrugsZsa Zsa FebryanaNo ratings yet
- Cardiac Emergencies PDFDocument57 pagesCardiac Emergencies PDFJohn Paulo CatacutanNo ratings yet
- Heart Disease JaninDocument7 pagesHeart Disease JaninTiara Anggun NurartoNo ratings yet
- Drugs Acting On Cardio Vascular SystemDocument16 pagesDrugs Acting On Cardio Vascular SystemANUSHYA B PSGRKCWNo ratings yet
- Payroll Management in Simhapuri HospitalsDocument30 pagesPayroll Management in Simhapuri HospitalsbhuvanaNo ratings yet
- Types of Cardiovascular Disease in The HeartDocument7 pagesTypes of Cardiovascular Disease in The Heartissey1652No ratings yet
- Aortic RegurgitationDocument19 pagesAortic RegurgitationsunilgenextNo ratings yet
- Cardiovascular Pharmacology ConceptsDocument11 pagesCardiovascular Pharmacology ConceptsHuney Kumar100% (1)
- A Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Ngaji Arrythmia Cordis 3Document122 pagesNgaji Arrythmia Cordis 3Dhita Dwi NandaNo ratings yet
- Cardiogenic Shock: Sparsh Goel 77Document28 pagesCardiogenic Shock: Sparsh Goel 77Sparsh GoelNo ratings yet
- Digitalis Toxicity Treatment and ManagementDocument39 pagesDigitalis Toxicity Treatment and ManagementAnonymous 3OoumAUytNo ratings yet
- The ABC's of Heart DiseaseDocument78 pagesThe ABC's of Heart DiseaseChRist LumingkewasNo ratings yet
- Review Literature Journal: Institute of Nursing EducationDocument12 pagesReview Literature Journal: Institute of Nursing EducationEr Shah Rukh QadriNo ratings yet
- Managing corticosteroids and their side effectsDocument6 pagesManaging corticosteroids and their side effectsKrista Madranca CastroNo ratings yet
- Heart Muscles, Valves & Blood Vessels (I)Document31 pagesHeart Muscles, Valves & Blood Vessels (I)Hussain GauharNo ratings yet
- AnginaDocument12 pagesAnginaDr-Sanjay SinghaniaNo ratings yet
- By: Prabhat Khare: Asst. ProfessorDocument25 pagesBy: Prabhat Khare: Asst. ProfessorSUMIT KUMAR PANDITNo ratings yet
- Common Drug InteractionsDocument1 pageCommon Drug InteractionsLuxs23No ratings yet
- Nursing Case Presentation For A Patient With CABG: Subject: Medical Surgical Nursing-IIDocument10 pagesNursing Case Presentation For A Patient With CABG: Subject: Medical Surgical Nursing-IIanamika sharmaNo ratings yet
- Associations USMLEDocument99 pagesAssociations USMLEnu.bombinaNo ratings yet
- Hepatic Failure & Hepatic EncephalopathyDocument37 pagesHepatic Failure & Hepatic Encephalopathyapi-19916399No ratings yet
- Cardiogenic ShockDocument6 pagesCardiogenic ShockhamadaelgenNo ratings yet
- Essential Hypertension ManagementDocument5 pagesEssential Hypertension Managementspicychips7No ratings yet
- PATHOPHYSIOLOGY OF SHOCKDocument56 pagesPATHOPHYSIOLOGY OF SHOCKDr. Haricharan ANo ratings yet
- Applying Pharmacology Concepts to Beta Blocker TherapyDocument269 pagesApplying Pharmacology Concepts to Beta Blocker TherapyTrishaNo ratings yet
- Ace Inhibutors MailDocument5 pagesAce Inhibutors MailWendy AdaoNo ratings yet
- Chest Tube, Urinary Catheter, Ryles Tube InsertionDocument60 pagesChest Tube, Urinary Catheter, Ryles Tube InsertionMohd Johari Mohd ShafuwanNo ratings yet
- Assessment or Acute Renal Failure SymptomsDocument6 pagesAssessment or Acute Renal Failure SymptomsRifa Aprillia CahyaniNo ratings yet
- Trends and Issues Affecting Nursing Practice-Newest S-16Document81 pagesTrends and Issues Affecting Nursing Practice-Newest S-16Lorraine CayamandaNo ratings yet
- Cardiac AsthmaDocument12 pagesCardiac AsthmaNeupane KsabNo ratings yet
- Valvular Heart DiseaseDocument2 pagesValvular Heart DiseaseAnonymous TVk12eX4No ratings yet
- Integrated Metabolism - 080144Document25 pagesIntegrated Metabolism - 080144Anand VeerananNo ratings yet
- Vitamin B12Document80 pagesVitamin B12Anand Veeranan100% (1)
- 9 Regulation of Blood GlucoseDocument47 pages9 Regulation of Blood GlucoseAnand VeerananNo ratings yet
- Reference ValueDocument2 pagesReference ValueAnand VeerananNo ratings yet
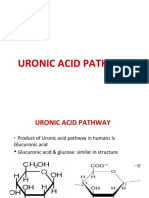
- 12 Uronic Acid PathwayDocument21 pages12 Uronic Acid PathwayAnand VeerananNo ratings yet
- Estimating Albumin ConcentrationDocument2 pagesEstimating Albumin ConcentrationAnand VeerananNo ratings yet
- Fructose Metabolism and Its RegulationDocument61 pagesFructose Metabolism and Its RegulationAnand Veeranan100% (1)
- Cell & Membrane Transport-1-3 - 091256Document138 pagesCell & Membrane Transport-1-3 - 091256Anand VeerananNo ratings yet
- 12 Monosaccharide METABOLISMDocument72 pages12 Monosaccharide METABOLISMAnand VeerananNo ratings yet
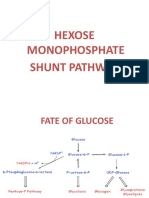
- Hexose Monophosphate Shunt PathwayDocument45 pagesHexose Monophosphate Shunt PathwayAnand VeerananNo ratings yet
- Cardiac BiomarkersDocument63 pagesCardiac BiomarkersAnand VeerananNo ratings yet
- Estimation of AlbuminDocument2 pagesEstimation of AlbuminAnand VeerananNo ratings yet
- Glucose Tolerance Test Definition: To Assess The Ability of The Body (Pancreas) To Handle A LoadDocument11 pagesGlucose Tolerance Test Definition: To Assess The Ability of The Body (Pancreas) To Handle A LoadAnand VeerananNo ratings yet
- Hormone ActionDocument142 pagesHormone ActionAnand Veeranan100% (1)
- Digestion & Absorption For Class 1Document56 pagesDigestion & Absorption For Class 1Anand VeerananNo ratings yet
- Fructosse Metabolism For ClassDocument50 pagesFructosse Metabolism For ClassAnand VeerananNo ratings yet
- Water As A ReagentDocument7 pagesWater As A ReagentAnand VeerananNo ratings yet
- Low Levels of Alkaline Phosphatase in The BloodDocument3 pagesLow Levels of Alkaline Phosphatase in The BloodAnand VeerananNo ratings yet
- Low Levels of Alkaline Phosphatase in The BloodDocument3 pagesLow Levels of Alkaline Phosphatase in The BloodAnand VeerananNo ratings yet
- Mass SpectrometryDocument64 pagesMass SpectrometryAnand VeerananNo ratings yet
- Biochemical CalculationsDocument458 pagesBiochemical CalculationsAnand VeerananNo ratings yet
- 1269Document9 pages1269Anand VeerananNo ratings yet
- Descendents of James WakefieldDocument19 pagesDescendents of James WakefieldiuchrisNo ratings yet
- Document1498792769575561 PDFDocument119 pagesDocument1498792769575561 PDFbajaj pulsar shitNo ratings yet
- Warcraft III World Editor Log File AnalysisDocument3 pagesWarcraft III World Editor Log File AnalysisJose Martin RoldanNo ratings yet
- Coberturax431paddiagun3master4 PDFDocument2 pagesCoberturax431paddiagun3master4 PDFMario TapiaNo ratings yet
- YMCA 2014 Fall Program GuideDocument20 pagesYMCA 2014 Fall Program GuideWWYMCANo ratings yet
- Osteo BallDocument7 pagesOsteo Ballcynneath305No ratings yet
- Advocate 13122022Document418 pagesAdvocate 13122022samarNo ratings yet
- Mario Kart CheatsDocument4 pagesMario Kart CheatsKrisNo ratings yet
- 2022 Presidential Scholars ProgramDocument8 pages2022 Presidential Scholars ProgramWKYC.comNo ratings yet
- TT WorkoutGuideDocument45 pagesTT WorkoutGuidedr rayyanNo ratings yet
- Don't Starve Together System Memory and Process Memory ReportDocument28 pagesDon't Starve Together System Memory and Process Memory ReportDiegoNo ratings yet
- Ultimate Gift Guide For Lotr 0 Hobbit FansDocument4 pagesUltimate Gift Guide For Lotr 0 Hobbit FansEnida MirnesNo ratings yet
- The Brabus Album.: Technomaniac Presents - .Document41 pagesThe Brabus Album.: Technomaniac Presents - .TechnomaniacNo ratings yet
- List of Products with PricesDocument1 pageList of Products with PricesPlay ProjectNo ratings yet
- Adududu Adadada AhahaDocument25 pagesAdududu Adadada AhahaWilkenn TuazonNo ratings yet
- Artificial Sports Lighting Design Guide 2012 051112Document61 pagesArtificial Sports Lighting Design Guide 2012 051112Mohamed FaragNo ratings yet
- A Folded PlateDocument10 pagesA Folded PlatePradnya ChavanNo ratings yet
- Mirror GuideDocument34 pagesMirror GuideIshtaraNo ratings yet
- Wirtgen Price List 2019 PDFDocument2,441 pagesWirtgen Price List 2019 PDFram singh70% (10)
- ISO Flanges & Components GuideDocument12 pagesISO Flanges & Components GuideJyoti Shankar MishraNo ratings yet
- Case Report of Three Patients With Wei-Flaccidity Syndrome Cured by Acupuncture-Moxibustion Therapy PDFDocument3 pagesCase Report of Three Patients With Wei-Flaccidity Syndrome Cured by Acupuncture-Moxibustion Therapy PDFtatodo1No ratings yet
- Lista PCDocument54 pagesLista PCFranklinOrtizNo ratings yet
- Main Switch Cab: TKB 00801-033 According DrawingDocument1 pageMain Switch Cab: TKB 00801-033 According DrawingMiller Andres ArocaNo ratings yet
- Pointers To Review in PE and HEALTH 11Document1 pagePointers To Review in PE and HEALTH 11Alkin RaymundoNo ratings yet
- How To Get AnDocument10 pagesHow To Get AnLaurențiu Grosu100% (1)
- January Month - Seva 2023Document3 pagesJanuary Month - Seva 2023saisri salesNo ratings yet
- Philosophy of Wing ChunDocument3 pagesPhilosophy of Wing Chungjh135No ratings yet
- Uk Rule Book 2ed Heroquest Board GameDocument10 pagesUk Rule Book 2ed Heroquest Board GameKieran DonohoeNo ratings yet
- Gale Force - Full Score PDFDocument62 pagesGale Force - Full Score PDFDougllas LopesNo ratings yet