You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Test 4: GRE Real 19Document6 pagesTest 4: GRE Real 19rdrprsdm2640No ratings yet
- Lab Guide #2 Coulombs LawDocument3 pagesLab Guide #2 Coulombs LawJoriel CruzNo ratings yet
- All The Questions of Section - A Are in Google Form and The Link To Attempt Them Is " Https://Forms - Gle/Jfvq8Wszicewchrj7 " 12 M Section - BDocument4 pagesAll The Questions of Section - A Are in Google Form and The Link To Attempt Them Is " Https://Forms - Gle/Jfvq8Wszicewchrj7 " 12 M Section - BKamal AnandNo ratings yet
- Firetroll User Interface Manual Ns550f-01-Instruction-manualDocument16 pagesFiretroll User Interface Manual Ns550f-01-Instruction-manualMike CerreroNo ratings yet
- Teaching Addition Facts PDFDocument75 pagesTeaching Addition Facts PDFsoraya gonzalezNo ratings yet
- List NotesDocument27 pagesList NotesMohit MauryaNo ratings yet
- Mechanical Damage and Fatigue Assessment of Dented Pipelines Using FeaDocument10 pagesMechanical Damage and Fatigue Assessment of Dented Pipelines Using FeaVitor lopesNo ratings yet
- Math 11-CORE Gen Math-Q2-Week 1Document26 pagesMath 11-CORE Gen Math-Q2-Week 1Christian GebañaNo ratings yet
- Change ManDocument17 pagesChange Mansrikanth9gannuNo ratings yet
- Experiment 08-A2dDocument3 pagesExperiment 08-A2dapi-277396867No ratings yet
- Bread and Pastry ProductionDocument9 pagesBread and Pastry Productionwhite newgatesNo ratings yet
- G3600 A4 Brochures PDFDocument4 pagesG3600 A4 Brochures PDFVictor NunezNo ratings yet
- Camber For Construction StageDocument18 pagesCamber For Construction StageOanh PhanNo ratings yet
- Column Design With ExcelDocument40 pagesColumn Design With ExcelMatiur Rahman BasumNo ratings yet
- Understanding The Relationship Between Human Behavior and Susceptibility To Cyber AttacksDocument25 pagesUnderstanding The Relationship Between Human Behavior and Susceptibility To Cyber AttacksVelibor SabanNo ratings yet
- An Empirical Study On The Nexus Between The Emotional Intelligence of Top Managers and Their Assessment of Intellectual CapitalDocument30 pagesAn Empirical Study On The Nexus Between The Emotional Intelligence of Top Managers and Their Assessment of Intellectual Capitalmaher76No ratings yet
- HKV-8 Valve Catalog SPLRDocument128 pagesHKV-8 Valve Catalog SPLRCabrera RodriguezNo ratings yet
- Chapter 1 - Distillation PDFDocument107 pagesChapter 1 - Distillation PDFFatin Natasha NazriNo ratings yet
- Defects in Stainless SteelDocument31 pagesDefects in Stainless SteelPrabhakar Kattula80% (5)
- VSF2 ND EdDocument345 pagesVSF2 ND EdRyanNo ratings yet
- Optimum Policy ControlDocument4 pagesOptimum Policy ControlKimberly VargasNo ratings yet
- Reading Report Student's Name: Leonel Lipa Cusi Teacher's Name: Maria Del Pilar, Quintana EspinalDocument2 pagesReading Report Student's Name: Leonel Lipa Cusi Teacher's Name: Maria Del Pilar, Quintana EspinalleonellipaNo ratings yet
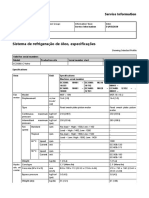
- Sistema de Refrigeração de Óleo, EspecificaçõesDocument2 pagesSistema de Refrigeração de Óleo, EspecificaçõesAlexandreNo ratings yet
- MICOM P12x-TechnicalDataSheetDocument28 pagesMICOM P12x-TechnicalDataSheetSeba GonzálezNo ratings yet
- NASA Facts Explorer XVI The Micrometeoroid SatelliteDocument4 pagesNASA Facts Explorer XVI The Micrometeoroid SatelliteBob AndrepontNo ratings yet
- Fpls 12 764103Document10 pagesFpls 12 764103Pawan MishraNo ratings yet
- CP IMarEst Mitigation of Corrosion by Cathodic ProtectionDocument25 pagesCP IMarEst Mitigation of Corrosion by Cathodic Protectionjose yoyNo ratings yet
- PDF 4.6 MDocument2 pagesPDF 4.6 MmdisicNo ratings yet
- Partial Differential Equations (Pdes)Document5 pagesPartial Differential Equations (Pdes)uploadingpersonNo ratings yet
- Stack008 V2Document1 pageStack008 V2Kryštof PaličkaNo ratings yet