You might also like
- Opioids Prescribed To Ohio Patients Decrease by 162 Million Doses Since 2012Document1 pageOpioids Prescribed To Ohio Patients Decrease by 162 Million Doses Since 2012Chris BurnsNo ratings yet
- DECEMBER 2016 Casino Revenue ReportDocument2 pagesDECEMBER 2016 Casino Revenue ReportChris BurnsNo ratings yet
- 2017 GasBuddy Fuel OutlookDocument19 pages2017 GasBuddy Fuel OutlookChris BurnsNo ratings yet
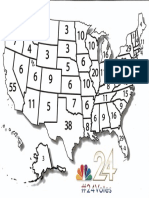
- NBC 24 Election MapDocument1 pageNBC 24 Election MapChris BurnsNo ratings yet
- Roasted Kohlrabi RecipeDocument1 pageRoasted Kohlrabi RecipeChris BurnsNo ratings yet
- 2016 17 New Strategies Addressing Infant Mortality in Ohio FINALDocument2 pages2016 17 New Strategies Addressing Infant Mortality in Ohio FINALChris BurnsNo ratings yet
- 2015 Ohio Infant Mortality Report FINALDocument12 pages2015 Ohio Infant Mortality Report FINALChris BurnsNo ratings yet
- Thanksgiving Meals in ToledoDocument1 pageThanksgiving Meals in ToledoChris BurnsNo ratings yet
- 2017 Proposed Budget Detail For The City of ToledoDocument203 pages2017 Proposed Budget Detail For The City of ToledoChris BurnsNo ratings yet
- 2017 Proposed Annual Operating Budget PDFDocument135 pages2017 Proposed Annual Operating Budget PDFChris BurnsNo ratings yet
- Thanksgiving Meals Offered Outside of ToledoDocument1 pageThanksgiving Meals Offered Outside of ToledoChris BurnsNo ratings yet
- City of Toledo Leaf Collection DatesDocument1 pageCity of Toledo Leaf Collection DatesChris BurnsNo ratings yet
- Wood County IssuesDocument3 pagesWood County IssuesChris BurnsNo ratings yet
- Lenawee County IssuesDocument53 pagesLenawee County IssuesChris BurnsNo ratings yet
- Lucas County Early VotingDocument1 pageLucas County Early VotingChris BurnsNo ratings yet
- Fulton County IssuesDocument1 pageFulton County IssuesChris BurnsNo ratings yet
- Putnam County Board of ElectionsDocument11 pagesPutnam County Board of ElectionsChris BurnsNo ratings yet
- Monroe County IssuesDocument12 pagesMonroe County IssuesChris BurnsNo ratings yet
- Lucas County General Election IssuesDocument1 pageLucas County General Election IssuesChris BurnsNo ratings yet
- Williams County IssuesDocument2 pagesWilliams County IssuesChris BurnsNo ratings yet
- Seneca County IssuesDocument7 pagesSeneca County IssuesChris BurnsNo ratings yet
- Lenawee County IssuesDocument53 pagesLenawee County IssuesChris BurnsNo ratings yet
- Paulding County IssuesDocument4 pagesPaulding County IssuesChris BurnsNo ratings yet
- Hancock County IssuesDocument7 pagesHancock County IssuesChris BurnsNo ratings yet
- Henry County IssuesDocument1 pageHenry County IssuesChris BurnsNo ratings yet
- Defiance IssuesDocument2 pagesDefiance IssuesChris BurnsNo ratings yet
- Ottawa County IssuesDocument1 pageOttawa County IssuesChris BurnsNo ratings yet
- Proposed Cut ListDocument2 pagesProposed Cut ListChris BurnsNo ratings yet
- Erie County IssuesDocument2 pagesErie County IssuesChris BurnsNo ratings yet
- RecipeDocument1 pageRecipeChris BurnsNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Health Teaching Plan HTNDocument3 pagesHealth Teaching Plan HTNCarpz Darpz88% (8)
- Introduction To QBD FixDocument25 pagesIntroduction To QBD FixAdel ZilviaNo ratings yet
- How Brain Science Can Inform Architectural DesignDocument12 pagesHow Brain Science Can Inform Architectural DesignadrianmoleavinNo ratings yet
- NTR OductionDocument83 pagesNTR OductionmalathiNo ratings yet
- Recurrent Gingival Cyst of Adult: A Rare Case Report With Review of LiteratureDocument5 pagesRecurrent Gingival Cyst of Adult: A Rare Case Report With Review of Literaturesayantan karmakarNo ratings yet
- Effectiveness of Planned Teaching Programme On The Knowledge of Endotracheal Suctioning Among Staff Nurses Working in IcuDocument6 pagesEffectiveness of Planned Teaching Programme On The Knowledge of Endotracheal Suctioning Among Staff Nurses Working in IcuRizwan KhanNo ratings yet
- In-process quality control of oral solid dosage formsDocument4 pagesIn-process quality control of oral solid dosage formsNur NabilahNo ratings yet
- B.A.,D.D.S.,M.S.D. : Herbert Werdlow, Bethesda, MDDocument7 pagesB.A.,D.D.S.,M.S.D. : Herbert Werdlow, Bethesda, MDMuchlis Fauzi ENo ratings yet
- OB Meds WorksheetDocument18 pagesOB Meds WorksheetrickyandsheenaNo ratings yet
- Ban Biblio NumberedDocument23 pagesBan Biblio NumberedYayangAsanggaNo ratings yet
- 9 Hair CleanseDocument11 pages9 Hair CleanseSeetha ChimakurthiNo ratings yet
- Estevan Jimenez Patient Clinical Report ForDocument7 pagesEstevan Jimenez Patient Clinical Report ForIsrael MelloNo ratings yet
- BONE Level 2-BDocument60 pagesBONE Level 2-Bjefri banjarnahorNo ratings yet
- Daily sales and expense recordsDocument29 pagesDaily sales and expense recordselsa fanny vasquez cepedaNo ratings yet
- Dental CementsDocument208 pagesDental CementsAkriti Goel33% (3)
- NIC Network HospitalsDocument172 pagesNIC Network HospitalsParas JainNo ratings yet
- PhysioEx Exercise 5 Activity 5Document3 pagesPhysioEx Exercise 5 Activity 5Gato100% (1)
- Cardiovascular SystemDocument10 pagesCardiovascular SystemitsmesuvekshaNo ratings yet
- Task Oriented Circuit Training Improves Ambulatory Functions in Acute Stroke A Randomized Controlled TrialDocument7 pagesTask Oriented Circuit Training Improves Ambulatory Functions in Acute Stroke A Randomized Controlled TrialadlestariNo ratings yet
- Cirugia BariatricaDocument9 pagesCirugia BariatricaedwardmenesesNo ratings yet
- Managing The Myths of Health Care PDFDocument5 pagesManaging The Myths of Health Care PDFkaremNo ratings yet
- How To Lower Your TriglyceridesDocument4 pagesHow To Lower Your TriglyceridesNoli CanlasNo ratings yet
- Top 10 Herbal Medicines in the PhilippinesDocument11 pagesTop 10 Herbal Medicines in the PhilippinesFritzie MacarayanNo ratings yet
- Unit 5 Drugs Acting On The Immune SystemDocument30 pagesUnit 5 Drugs Acting On The Immune SystemBea Bianca Cruz100% (1)
- MycologyDocument17 pagesMycologyRachana PurohitNo ratings yet
- Clubfoot Definition, Types, and TreatmentDocument5 pagesClubfoot Definition, Types, and TreatmentcrisolandNo ratings yet
- Assessment of Antimicrobial Activity of Cassia Fistula and Flacoartia Indica Leaves.Document5 pagesAssessment of Antimicrobial Activity of Cassia Fistula and Flacoartia Indica Leaves.Eliana CaraballoNo ratings yet
- Oral Physio FinalDocument34 pagesOral Physio FinaldraggarwalNo ratings yet
- Digital Paper Trail DPTDocument5 pagesDigital Paper Trail DPTapi-549372008No ratings yet
- Public Notice Dated 16.11.2018-Disability-AppendixHDocument4 pagesPublic Notice Dated 16.11.2018-Disability-AppendixHDisability Rights AllianceNo ratings yet