You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Jurnal Sag-46-2-23-1411-102Document8 pagesJurnal Sag-46-2-23-1411-102Carolina SalimNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- American Burn Association Concensus Definition On Burn SepsisDocument1 pageAmerican Burn Association Concensus Definition On Burn SepsisCarolina SalimNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Dia Care 2001 Haymond 643 5Document3 pagesDia Care 2001 Haymond 643 5Carolina SalimNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
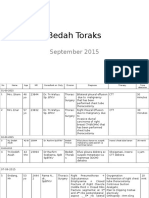
- Toraks Sep15Document11 pagesToraks Sep15Carolina SalimNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Urologi Sep15Document8 pagesUrologi Sep15Carolina SalimNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Bahan Presentasi QPS-PMKP Untuk Champion PPDS 2015 Newest AugustDocument49 pagesBahan Presentasi QPS-PMKP Untuk Champion PPDS 2015 Newest AugustCarolina SalimNo ratings yet
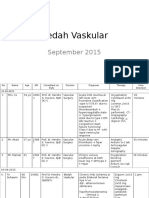
- Vaskular Sep15 RSHSDocument6 pagesVaskular Sep15 RSHSCarolina SalimNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- UB HSPED Differential Diagnosis of Lower Back PainDocument62 pagesUB HSPED Differential Diagnosis of Lower Back PainJolaine ValloNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- MSDS KleratDocument4 pagesMSDS KleratSadhana Sentosa100% (2)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- University of Cambridge Local Examinations Syndicate Biomedical Admissions TestDocument20 pagesUniversity of Cambridge Local Examinations Syndicate Biomedical Admissions TestNeil SahooNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Screening For Colorectal CancerDocument6 pagesScreening For Colorectal CancerDiana BlanaruNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- 3rd Ed General Cheat Sheet PDFDocument9 pages3rd Ed General Cheat Sheet PDFAlan RideoutNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Ayurveda Medicine of the GodsDocument20 pagesAyurveda Medicine of the Godsramdas2430No ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- Cambridge Food HygieneDocument22 pagesCambridge Food Hygieneapi-350003268No ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Applied PalynologyDocument2 pagesApplied PalynologySanjoy NingthoujamNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Medical Physics - RespiratoryDocument9 pagesMedical Physics - RespiratoryAhmad wastiNo ratings yet
- 12 Biology Notes Ch11 Biotechnology Principles and ProcessesDocument9 pages12 Biology Notes Ch11 Biotechnology Principles and ProcessesAnkit YadavNo ratings yet
- Garlic - Toxic and A Brain Synchronization DestroyerDocument6 pagesGarlic - Toxic and A Brain Synchronization Destroyerxreader0No ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Aonla: Aonla (Emblica Officinalis) or Indian Gooseberry Is Indigenous To Indian Sub-Continent. India Ranks First inDocument21 pagesAonla: Aonla (Emblica Officinalis) or Indian Gooseberry Is Indigenous To Indian Sub-Continent. India Ranks First inphani kumarNo ratings yet
- CSH Perspectives Rev - Apolipoprotein E and Apolipoprotein E Receptors - Normal Biology and Roles in ADDocument23 pagesCSH Perspectives Rev - Apolipoprotein E and Apolipoprotein E Receptors - Normal Biology and Roles in ADGeneziz DiazNo ratings yet
- DEPRESSIONDocument2 pagesDEPRESSIONgracerroa13No ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Hesi Hints Part 4Document2 pagesHesi Hints Part 4Sharon TanveerNo ratings yet
- Alkalizing Nutritional Therapy in The Prevention and Treatment of Any Cancerous Condition by Robert Young Galina Migalko (Young, Robert Migalko, Galina)Document51 pagesAlkalizing Nutritional Therapy in The Prevention and Treatment of Any Cancerous Condition by Robert Young Galina Migalko (Young, Robert Migalko, Galina)Maria S100% (1)
- 2021 Book EmergingTrendsInPlantPathologyDocument849 pages2021 Book EmergingTrendsInPlantPathologyMayra GameroNo ratings yet
- Antiviral Viral Compound From Streptomyces Ghanaensis Like Strain Against White Spot Syndrome Virus (WSSV) of ShrimpDocument59 pagesAntiviral Viral Compound From Streptomyces Ghanaensis Like Strain Against White Spot Syndrome Virus (WSSV) of ShrimpkannalijayaNo ratings yet
- Crohn's Disease - A Medical Astrology ExaminationDocument3 pagesCrohn's Disease - A Medical Astrology ExaminationPRADEEP MUTHUKULAMNo ratings yet
- Effect of Cinnamon On Diabetes Mariana Kalenichenko University of North Florida FOS 4041 April 3rd, 2018Document11 pagesEffect of Cinnamon On Diabetes Mariana Kalenichenko University of North Florida FOS 4041 April 3rd, 2018api-435685106No ratings yet
- Ptosis SurgeryDocument18 pagesPtosis Surgerysri sinagaNo ratings yet
- Lesson 3 Gas ExchangeDocument7 pagesLesson 3 Gas ExchangeBrent PatarasNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- ICD 10 Codes For Neurology-MI4957Document6 pagesICD 10 Codes For Neurology-MI4957fkuii2009No ratings yet
- Unit Test 8B: Are Girls Better at Cooking?Document5 pagesUnit Test 8B: Are Girls Better at Cooking?Ana TodorovićNo ratings yet
- Solutions For Bronchoscopy Brochure 0001 v1 en 2012Document13 pagesSolutions For Bronchoscopy Brochure 0001 v1 en 2012Monica PetreNo ratings yet
- Medif Information Sheet For Passengers Requiring Medical Clearence - Part 1-2 - Tarom From 4122 - 2Document2 pagesMedif Information Sheet For Passengers Requiring Medical Clearence - Part 1-2 - Tarom From 4122 - 2ViolleteMorenaNo ratings yet
- Spring 2014 IPG Spanish TitlesDocument68 pagesSpring 2014 IPG Spanish TitlesIndependent Publishers GroupNo ratings yet
- Hypoxia: Deficiency in Oxygen Delivery or Utilization at Tissue LevelDocument37 pagesHypoxia: Deficiency in Oxygen Delivery or Utilization at Tissue LevelandrenicholastobingNo ratings yet
- Research Paper On Sweet PotatoDocument7 pagesResearch Paper On Sweet Potatoafeawldza100% (1)
- June 2018 QP - Biology 1 (H) Edexcel Science GCSEDocument24 pagesJune 2018 QP - Biology 1 (H) Edexcel Science GCSESHOABNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)