You might also like
- Frequences RifeDocument294 pagesFrequences Rifedoggydog100% (5)
- Hemodialysis and Peritoneal DialysisDocument43 pagesHemodialysis and Peritoneal DialysisGulshanNo ratings yet
- Case Presentation: - Vuppu BhavaniDocument53 pagesCase Presentation: - Vuppu BhavaniLohith Kumar MenchuNo ratings yet
- History Taking: DR Anwar H. SiddiquiDocument26 pagesHistory Taking: DR Anwar H. SiddiquiAssad mustafNo ratings yet
- Sample SOAP NoteDocument6 pagesSample SOAP NoteLorrie83% (6)
- CASE 3 MEDICINE JULY 10 2019 AcutePyeloDocument15 pagesCASE 3 MEDICINE JULY 10 2019 AcutePyeloTrisNo ratings yet
- History and Physical Examination 2014 11 13 00 25 21 UtcDocument7 pagesHistory and Physical Examination 2014 11 13 00 25 21 Utcapi-310557802No ratings yet
- A Simple Guide to Parathyroid Disorders, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Parathyroid Disorders, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Neurological Soap NoteDocument10 pagesNeurological Soap Notesara walterNo ratings yet
- SOAP Note NSG 6420 Week 8Document6 pagesSOAP Note NSG 6420 Week 8Jan FloydNo ratings yet
- Duck ProductionDocument10 pagesDuck ProductionSamuel Ivan Ngan100% (1)
- Sample SoapDocument9 pagesSample SoapDouglas Greg Cook90% (20)
- Emerging DiseaseDocument68 pagesEmerging DiseaseIwan Purnawan100% (1)
- Pediatric Osce History and Communication Checklist-1Document90 pagesPediatric Osce History and Communication Checklist-1Sabera Kapasi100% (1)
- History & Physical ExaminationDocument67 pagesHistory & Physical ExaminationDiggi VioNo ratings yet
- Health Indicators FormulasDocument2 pagesHealth Indicators Formulaskristinetan21No ratings yet
- Final Assessment Soap NoteDocument13 pagesFinal Assessment Soap Noteapi-494643478100% (3)
- Human Papillomavirus: Divine Word College of Laoag School of Basic Education High SchoolDocument10 pagesHuman Papillomavirus: Divine Word College of Laoag School of Basic Education High SchoolYzabel MacadangdangNo ratings yet
- Soap RoutineDocument3 pagesSoap RoutineRoberto Ramos100% (1)
- Low Back PainDocument9 pagesLow Back PainDoc AchondoNo ratings yet
- SLE Test Samples by SCHSDocument207 pagesSLE Test Samples by SCHSSyeda Mariyam Zehra83% (6)
- Neuro Case StudyDocument28 pagesNeuro Case StudyRa Mee LahNo ratings yet
- Final Practicum - Soap Note 2Document19 pagesFinal Practicum - Soap Note 2api-494643478No ratings yet
- Case DiscussionDocument8 pagesCase DiscussionAishwarya BharathNo ratings yet
- General PE Case Write-Up - Doctoring IIIDocument5 pagesGeneral PE Case Write-Up - Doctoring IIIchristietwongNo ratings yet
- SOAP Older Well WomanDocument11 pagesSOAP Older Well Womanniknshell100% (1)
- Case Write-Up 1Document16 pagesCase Write-Up 1Zharif Fikri100% (3)
- Nurs 5018 - Soap Note Well-Woman ExamDocument7 pagesNurs 5018 - Soap Note Well-Woman Examapi-308904543No ratings yet
- H&P - Sample - Complete ExamDocument7 pagesH&P - Sample - Complete ExamNicole Brassington100% (4)
- Clinical Case PresentationDocument44 pagesClinical Case PresentationRUSSELL CILOTNo ratings yet
- Infection Control GuidelinesDocument48 pagesInfection Control GuidelinesdrlaithmNo ratings yet
- Adult Medical SOAP NoteDocument4 pagesAdult Medical SOAP NoteBhanu100% (6)
- DR - Umpierrere2012 2013 4Document70 pagesDR - Umpierrere2012 2013 4Roberto RamosNo ratings yet
- Health AssessmentDocument26 pagesHealth AssessmentBlake Kammin100% (1)
- A For and Against EssayDocument4 pagesA For and Against Essayluciana20straNo ratings yet
- Family Medicine - General Practice MEQ 2006Document6 pagesFamily Medicine - General Practice MEQ 2006jermie22100% (1)
- Case Study MM-2Document40 pagesCase Study MM-2Aya Sayed100% (1)
- Final Practicum - Soap Note 1Document16 pagesFinal Practicum - Soap Note 1api-49464347867% (3)
- USP 51 Antimicrobial Effectiveness TestDocument4 pagesUSP 51 Antimicrobial Effectiveness TestAki Espaldon100% (1)
- 4th Medi Pulmo Apr 15 - 17, 2021 QuestionsDocument22 pages4th Medi Pulmo Apr 15 - 17, 2021 QuestionsSheda BondNo ratings yet
- History TakingDocument9 pagesHistory Takingmahmoud selimNo ratings yet
- Grand RoundDocument81 pagesGrand RoundMustofa HusainNo ratings yet
- Audio File 16 - Syed RizwanDocument6 pagesAudio File 16 - Syed RizwansayyedrindianNo ratings yet
- Dysuria: Name: Chathiya Banu M/Num: MBBS 1608-7368Document39 pagesDysuria: Name: Chathiya Banu M/Num: MBBS 1608-7368Chathiya Banu KrishenanNo ratings yet
- AnasarcaDocument54 pagesAnasarcaSulaiman TahsinNo ratings yet
- LinksDocument24 pagesLinksTrisNo ratings yet
- Clinicalmeetingoriginal 161117192705Document50 pagesClinicalmeetingoriginal 1611171927057dbnf4stjyNo ratings yet
- Name: Onipha Tappin DATE: 31 OCTOBER, 2012 Teacher: Is Francis Subject: Health AssessmentDocument26 pagesName: Onipha Tappin DATE: 31 OCTOBER, 2012 Teacher: Is Francis Subject: Health AssessmentNichola TappinNo ratings yet
- Clerk GCPDocument19 pagesClerk GCPNikki DiocampoNo ratings yet
- Preparation For Paces: HistoryDocument37 pagesPreparation For Paces: HistoryalaaNo ratings yet
- Kampala International University:: Morebu Peter MomanyiDocument10 pagesKampala International University:: Morebu Peter Momanyifadila mohammedNo ratings yet
- Pediatric Surgery Case Taking Notes: Dr. Anusiri InugalaDocument44 pagesPediatric Surgery Case Taking Notes: Dr. Anusiri InugalaAshwin KumarNo ratings yet
- "Don't Take My Breath Away" A Case Presentation On Pneumocystis PneumoniaDocument20 pages"Don't Take My Breath Away" A Case Presentation On Pneumocystis PneumoniaNikki DiocampoNo ratings yet
- History Taking2Document25 pagesHistory Taking2Capture UnseenNo ratings yet
- Case Presentation: StrokeDocument27 pagesCase Presentation: StrokeHemant ShahNo ratings yet
- Surg Week 4Document75 pagesSurg Week 4Casey YanoNo ratings yet
- SOAP - Blank - Template Word Doc 2022Document6 pagesSOAP - Blank - Template Word Doc 2022Joan McutestNo ratings yet
- Weekly Patient Report FormDocument8 pagesWeekly Patient Report FormOsama FrancisNo ratings yet
- Utility of Bogers Approach in Treating A Casee of Nephrotic Syndrome, Evidence Based Case ReportDocument4 pagesUtility of Bogers Approach in Treating A Casee of Nephrotic Syndrome, Evidence Based Case Reportsri harithaNo ratings yet
- Anesthesia PLANDocument6 pagesAnesthesia PLANJawad khanNo ratings yet
- Soap Note TemplateDocument4 pagesSoap Note TemplateAdamNo ratings yet
- Medicine CasesDocument56 pagesMedicine Casesmohamed muhsinNo ratings yet
- Nephrotic SyndromeDocument61 pagesNephrotic SyndromeRanah Julia Garchitorena AyoNo ratings yet
- HHD 9 Accident EmergencyDocument6 pagesHHD 9 Accident Emergencymusy9999No ratings yet
- Pae-Central Nervous SystemDocument17 pagesPae-Central Nervous SystemMegha ProjectsNo ratings yet
- Carbuncle, Incision, Drainage, DebridementDocument11 pagesCarbuncle, Incision, Drainage, DebridementAlvin Germo PasuquinNo ratings yet
- Mustansiriyah Lecture Notes On Surgical History & Clinical ExaminationDocument57 pagesMustansiriyah Lecture Notes On Surgical History & Clinical Examinationنور الهدى ابراهيم خضير معيليNo ratings yet
- CASE STUDY Lung Ca With Pleural EffDocument8 pagesCASE STUDY Lung Ca With Pleural EffL4 CLERK - UY, Rhea Andrea F.No ratings yet
- Isack InternalDocument10 pagesIsack InternalisacksotiNo ratings yet
- H&P - Sample - Partial ExamDocument6 pagesH&P - Sample - Partial Exam808kailuaNo ratings yet
- Emedley Practice/ Guidelines: JaniceDocument13 pagesEmedley Practice/ Guidelines: JaniceRupsyNo ratings yet
- History: Chief Complaint: History of Present Illness: Patient Is A 59 Year Old G6 P1051 Woman Who Is An Inmate That WasDocument9 pagesHistory: Chief Complaint: History of Present Illness: Patient Is A 59 Year Old G6 P1051 Woman Who Is An Inmate That WasRoberto RamosNo ratings yet
- Paciente 3Document80 pagesPaciente 3Roberto RamosNo ratings yet
- Universidad Puerto Rico Manual 1415Document161 pagesUniversidad Puerto Rico Manual 1415Roberto RamosNo ratings yet
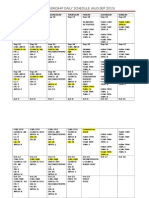
- Ob-Gyn Clerkship Daily Schedule (Aug-Sep 2015)Document3 pagesOb-Gyn Clerkship Daily Schedule (Aug-Sep 2015)Roberto RamosNo ratings yet
- HTTPDocument1 pageHTTPRoberto RamosNo ratings yet
- Organic NZ May 01 2018Document68 pagesOrganic NZ May 01 2018Salva GarcíaNo ratings yet
- Enfermedades EmergentesDocument216 pagesEnfermedades EmergentesCaaarolNo ratings yet
- EU Digital COVID Certificate Certifikát EU COVID-19: Czech RepublicDocument1 pageEU Digital COVID Certificate Certifikát EU COVID-19: Czech Republickrasota izdorovieNo ratings yet
- Complete List of Vaccines 2016Document8 pagesComplete List of Vaccines 2016Evangelist Michelle Leavy-BreunigNo ratings yet
- Vaxbrochure 012017Document2 pagesVaxbrochure 012017api-414476993No ratings yet
- Diagnostic Assays & Instruments: Gold Standard Diagnostics Europe 2022 International CatalogueDocument28 pagesDiagnostic Assays & Instruments: Gold Standard Diagnostics Europe 2022 International CatalogueMentor KurshumliuNo ratings yet
- Improved Chicken RearingDocument4 pagesImproved Chicken RearingAnonymous asCQ7N7GVNo ratings yet
- A Brief History of VaccinationDocument1 pageA Brief History of Vaccinationshennie anteNo ratings yet
- Cap Guidelines 2010Document42 pagesCap Guidelines 2010Marion Andrea PoblacionNo ratings yet
- CertificateDocument1 pageCertificateVikas Sharma (205663)No ratings yet
- NCM 107 Newborn SkillsDocument5 pagesNCM 107 Newborn Skillsevangdelacruz1010No ratings yet
- Health Facility Micro Plan-2Document14 pagesHealth Facility Micro Plan-2Peter KlaniNo ratings yet
- BRY's Microbiology, 1st SemesterDocument95 pagesBRY's Microbiology, 1st SemesterSaima ZuberiNo ratings yet
- (Edit) Signs and Symptoms: Typhoid FeverDocument10 pages(Edit) Signs and Symptoms: Typhoid FeverAudita LeeNo ratings yet
- Capstone Essay-2Document10 pagesCapstone Essay-2api-460858215No ratings yet
- Zenius Un 2017Document39 pagesZenius Un 2017dindaNo ratings yet
- Communicable Disease: List of Communicable DiseasesDocument13 pagesCommunicable Disease: List of Communicable DiseasesjasmineNo ratings yet
- Awareness and PreventionDocument24 pagesAwareness and Preventionnoname0% (1)
- DR Nur Farhanah SPPD - Penggunaan AB Rasional 1 PDFDocument16 pagesDR Nur Farhanah SPPD - Penggunaan AB Rasional 1 PDFFlorantia Setya NugrohoNo ratings yet
- Maklumat Vaksinasi: Vaccination DetailsDocument2 pagesMaklumat Vaksinasi: Vaccination Detailsahmad hussainiNo ratings yet