You might also like
- Algo Acs PDFDocument1 pageAlgo Acs PDFJim Christian EllaserNo ratings yet
- Acut Coronary SyndromesDocument1 pageAcut Coronary SyndromesMuhittin Selçuk ÖzkanNo ratings yet
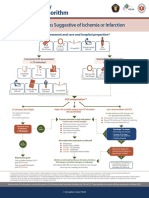
- Syndroms Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PrepartionDocument1 pageSyndroms Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PrepartionAnonymous CKAborxxwNo ratings yet
- Syndroms Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PrepartionDocument8 pagesSyndroms Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PrepartionNugroho TeguhNo ratings yet
- Syndromes Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PreparationDocument1 pageSyndromes Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PreparationIGOR SHEYNINNo ratings yet
- Syndromes Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PreparationDocument1 pageSyndromes Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital Preparationgusti angri angalanNo ratings yet
- Posters For ClinicDocument80 pagesPosters For ClinicdenzkissaieNo ratings yet
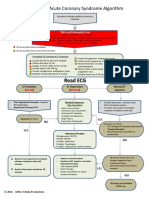
- Acute Coronary Syndromes Algorithm: Patient Has Signs Suggestive of Ischemia or InfarctionDocument1 pageAcute Coronary Syndromes Algorithm: Patient Has Signs Suggestive of Ischemia or Infarctionjohndoe1995No ratings yet
- Acs PDFDocument1 pageAcs PDFPowool LalaNo ratings yet
- Reanimacion CardiopulmonarDocument15 pagesReanimacion CardiopulmonarVictoriano ValienteNo ratings yet
- Algorithm 1: Initial Evaluation and Management: Symptoms of Possible ACSDocument6 pagesAlgorithm 1: Initial Evaluation and Management: Symptoms of Possible ACSNenyNo ratings yet
- Emergency Department STEMI Algorithm GuideDocument1 pageEmergency Department STEMI Algorithm GuideOgizWaraNo ratings yet
- Tachycardia AlgorithmDocument1 pageTachycardia AlgorithmGideon BahuleNo ratings yet
- Pediatric Bradycardia With A Pulse and Poor Perfusion AlgorithmDocument1 pagePediatric Bradycardia With A Pulse and Poor Perfusion AlgorithmRadhiatul MardhiahNo ratings yet
- Stemi NSTEMI or Unstable Angina: Offer AspirinDocument1 pageStemi NSTEMI or Unstable Angina: Offer AspirinVemuri SrinivasNo ratings yet
- AlgorithmACLStachycardiawithapulse PDFDocument1 pageAlgorithmACLStachycardiawithapulse PDFDendy Frannuzul RamadhanNo ratings yet
- Tachycardia With A Pulse Algorithm: Assess Appropriateness For Clinical ConditionDocument1 pageTachycardia With A Pulse Algorithm: Assess Appropriateness For Clinical ConditionDendy Frannuzul RamadhanNo ratings yet
- ACLS ReportDocument58 pagesACLS ReportCamille Honeyleith FernandoNo ratings yet
- ACLS Simplify AlgorithmDocument6 pagesACLS Simplify AlgorithmKristine Monforte Coma UritaNo ratings yet
- Adult Tachycardia (With Pulse) AlgorithmDocument1 pageAdult Tachycardia (With Pulse) AlgorithmJames ChoiNo ratings yet
- UNC ED Code Stroke Pathway 9 2016 FINALDocument2 pagesUNC ED Code Stroke Pathway 9 2016 FINALJackNo ratings yet
- EMS Chest Pain ACS GuidelinesDocument1 pageEMS Chest Pain ACS GuidelinesJuanaly BadiolaNo ratings yet
- Algoritma Ambulance - PHCDocument11 pagesAlgoritma Ambulance - PHCYassarNo ratings yet
- Assess Appropriateness For Clinical Condition. Heart Rate Typically 150/min If TachyarrhythmiaDocument1 pageAssess Appropriateness For Clinical Condition. Heart Rate Typically 150/min If TachyarrhythmiaSiti Nur R Firda FauziyahNo ratings yet
- Algorithm of Resuscitation CareDocument1 pageAlgorithm of Resuscitation CarejyothiNo ratings yet
- Algo ArrestDocument2 pagesAlgo ArrestLocomotorica FK UkiNo ratings yet
- ACLS 2015 Algorithm and Anesthesia ACLS PDFDocument14 pagesACLS 2015 Algorithm and Anesthesia ACLS PDFTaufiqurrahman RizkiNo ratings yet
- AiepiDocument12 pagesAiepiRenzo Iván Marín DávalosNo ratings yet
- AlgorithmACLS Tachycardia 200612Document1 pageAlgorithmACLS Tachycardia 200612YassarNo ratings yet
- ACS Algorithm 2016 PDFDocument1 pageACS Algorithm 2016 PDFrabin1994No ratings yet
- Acute Coronary SyndromeDocument7 pagesAcute Coronary SyndromePuskesmas Pinang JayaNo ratings yet
- Cardiac Arrest Circular AlgorithmDocument2 pagesCardiac Arrest Circular AlgorithmJunius SimarmataNo ratings yet
- Peri-Arrest ArrythmiaDocument14 pagesPeri-Arrest Arrythmiamohamed mowafeyNo ratings yet
- AdultTachycardiaWithPulse AlgorithmDocument1 pageAdultTachycardiaWithPulse AlgorithmIsmail SlimNo ratings yet
- G2015 Adult Tachycardia PDFDocument1 pageG2015 Adult Tachycardia PDFibbs91No ratings yet
- G2015 Adult Tachycardia PDFDocument1 pageG2015 Adult Tachycardia PDFPlabber JuneNo ratings yet
- Ecg ReadingsDocument11 pagesEcg ReadingsAnton Laurenciana100% (5)
- Start CPR Shout For Help/Activate Emergency Response: Give Oxygen Attach Monitor/DefibrillatorDocument2 pagesStart CPR Shout For Help/Activate Emergency Response: Give Oxygen Attach Monitor/DefibrillatorFelicia ErikaNo ratings yet
- Algorithm-ACLS ACS 200806 1Document1 pageAlgorithm-ACLS ACS 200806 1Kavya Shree100% (1)
- Acute Coronary SyndromeDocument5 pagesAcute Coronary Syndromecotten joeNo ratings yet
- ACLS ACS Algorithm NewDocument3 pagesACLS ACS Algorithm Newsambo100% (1)
- Advanced Life Support Algorithm: Learning OutcomesDocument8 pagesAdvanced Life Support Algorithm: Learning OutcomesParvathy R NairNo ratings yet
- Algo Tachycardia PDFDocument1 pageAlgo Tachycardia PDFYudhistira AdiNo ratings yet
- Cardiac Arrest Circular AlgorhythmDocument4 pagesCardiac Arrest Circular AlgorhythmAisyah Nur KarimahNo ratings yet
- ACLS Protocols Pocket VersionDocument2 pagesACLS Protocols Pocket Versionjohndoe1995No ratings yet
- Acute Coronary Syndromes - HandoutDocument4 pagesAcute Coronary Syndromes - Handoutapi-641524095No ratings yet
- Diagnosis and Initial Treatment of Ischemic Stroke: Health Care GuidelineDocument62 pagesDiagnosis and Initial Treatment of Ischemic Stroke: Health Care GuidelineIrsyah Dwi RNo ratings yet
- Chest Pain System - DisorderDocument1 pageChest Pain System - DisorderAA DDNo ratings yet
- Inpatientpathway PDFDocument2 pagesInpatientpathway PDFLuis Fernando SaraviaNo ratings yet
- Diagnosis and Initial Treatment of Ischemic Stroke: Health Care GuidelineDocument71 pagesDiagnosis and Initial Treatment of Ischemic Stroke: Health Care GuidelineRosyid PrasetyoNo ratings yet
- Expanding The Therapeutic Window For Acute Ischemic Stroke:: New Agents, New ApproachesDocument29 pagesExpanding The Therapeutic Window For Acute Ischemic Stroke:: New Agents, New ApproachesDr. RajibNo ratings yet
- Acs With New Stemi GuidelineDocument35 pagesAcs With New Stemi Guidelinematmin07No ratings yet
- ACLS Advanced Cardiovascular Life Support Provider Manual 2023From EverandACLS Advanced Cardiovascular Life Support Provider Manual 2023No ratings yet
- Health 10 LAS Q4Document19 pagesHealth 10 LAS Q4JOSH ELORDENo ratings yet
- The PICOT Method - Why and How v4 - CADocument3 pagesThe PICOT Method - Why and How v4 - CAmelodia gandezaNo ratings yet
- G2 NCM 101 - HygieneDocument42 pagesG2 NCM 101 - HygieneItzayana SyNo ratings yet
- Wound Dressing: Anatomy, Classification, Healing and Debridement Methods/TITLEDocument43 pagesWound Dressing: Anatomy, Classification, Healing and Debridement Methods/TITLENik FatihahNo ratings yet
- Review Notes for Diabetes Mellitus Types, Pathophysiology, Complications & ManagementDocument8 pagesReview Notes for Diabetes Mellitus Types, Pathophysiology, Complications & ManagementEditha LucasNo ratings yet
- Pablo de Egina, Medicina 2Document536 pagesPablo de Egina, Medicina 2ataulfNo ratings yet
- Understanding HIV/AIDS: Causes, Symptoms, PreventionDocument17 pagesUnderstanding HIV/AIDS: Causes, Symptoms, PreventionphilNo ratings yet
- What Is Good Practice in Autism EducationDocument51 pagesWhat Is Good Practice in Autism EducationAinisaNo ratings yet
- BCB 411 - Lec 2Document15 pagesBCB 411 - Lec 2NaushinKhanNo ratings yet
- Running Head: Victim Turned Bully 1Document17 pagesRunning Head: Victim Turned Bully 1JUDY ANNNo ratings yet
- EAT 208 Environmental Law, Health and Safety SEMESTER 2, 2020/2021Document14 pagesEAT 208 Environmental Law, Health and Safety SEMESTER 2, 2020/2021Suganyah RajuNo ratings yet
- Worksheets 5Document4 pagesWorksheets 5LEILA SILVESTRENo ratings yet
- ThesisDocument44 pagesThesisApple T. ElarcosaNo ratings yet
- 811 2Document16 pages811 2almightyx10No ratings yet
- USAID Impact of Health Systems Strengthening On HealthDocument66 pagesUSAID Impact of Health Systems Strengthening On HealthMamadou Selly LyNo ratings yet
- Agep Poster EadvDocument1 pageAgep Poster EadvAhmet KayaaltıNo ratings yet
- DR. SEBI BIBLE (Stewart, Angela)Document691 pagesDR. SEBI BIBLE (Stewart, Angela)griffindolphNo ratings yet
- نموذج امتحان مزاولة مهنة الصيدلة16-7-2009Document13 pagesنموذج امتحان مزاولة مهنة الصيدلة16-7-2009Ahmed Fouad100% (2)
- DR Burns Mood InventoryDocument2 pagesDR Burns Mood InventoryEana Jamaica MadriñanNo ratings yet
- Smile DesignDocument104 pagesSmile DesignEazhil Raj100% (3)
- Leveling and Aligning Challenges and SolutionsDocument21 pagesLeveling and Aligning Challenges and SolutionsYaser JasNo ratings yet
- (Nutrition and Health) Ted Wilson, Norman J. Temple, George A. Bray - Nutrition Guide For Physicians and Related Healthcare Professions-Humana (2022)Document485 pages(Nutrition and Health) Ted Wilson, Norman J. Temple, George A. Bray - Nutrition Guide For Physicians and Related Healthcare Professions-Humana (2022)Guillermo Hernandez100% (3)
- Diabetic Retinopathy FinalDocument17 pagesDiabetic Retinopathy FinalHemant MallahNo ratings yet
- Nursing Care Plan - Risk For BleedingDocument2 pagesNursing Care Plan - Risk For BleedingDaniel Andre S. SomorayNo ratings yet
- Test Bank For Psychiatric Mental Health Nursing 4th Edition by FrischDocument22 pagesTest Bank For Psychiatric Mental Health Nursing 4th Edition by Frischmaxwelljoneswojxafndsk100% (45)
- Rehabilitation Conceptual FrameworkDocument17 pagesRehabilitation Conceptual FrameworkShikha SagarNo ratings yet
- Kisi Kisi RANYADocument17 pagesKisi Kisi RANYAmikel haluNo ratings yet
- Risk For Unstable Blood Glucose Related To Unhealthy Lifestyle.Document8 pagesRisk For Unstable Blood Glucose Related To Unhealthy Lifestyle.eleinsamNo ratings yet
- Health Optimizing Physical Education-Quarter 4 (Module 4)Document6 pagesHealth Optimizing Physical Education-Quarter 4 (Module 4)Shanghai Ni Yoshinori100% (1)
- Taking Care of The Respiratory SystemDocument8 pagesTaking Care of The Respiratory SystemAceNo ratings yet