You might also like
- A Simple Guide To Tooth Whitening: The Dental Learning NetworkDocument28 pagesA Simple Guide To Tooth Whitening: The Dental Learning NetworkNur AwanisNo ratings yet
- Local Anesthetic ReviewDocument43 pagesLocal Anesthetic ReviewJannyl GonzalesNo ratings yet
- Tooth Erosion: Risk Factors and Therapeutics: The Dental Learning NetworkDocument30 pagesTooth Erosion: Risk Factors and Therapeutics: The Dental Learning Networkmsaber1No ratings yet
- Medical Emergencies in Dental OfficeDocument37 pagesMedical Emergencies in Dental Officeleozee100% (2)
- ADC Written Exam Handbook DHDTDocument16 pagesADC Written Exam Handbook DHDTAli Raza Munir AhmadNo ratings yet
- AGDI Enrolment FormDocument4 pagesAGDI Enrolment FormHemlata GuptaNo ratings yet
- Basic Ethics in DentistryDocument30 pagesBasic Ethics in Dentistryਕੋਮਲ ਮੱਲਾਂਵਾਲੀਆNo ratings yet
- Well Ap: Candidate HandbookDocument23 pagesWell Ap: Candidate HandbookzairazaidiNo ratings yet
- Medical Assistant Practice Exam 750 2015 PDFDocument433 pagesMedical Assistant Practice Exam 750 2015 PDFThanaa85% (89)
- School of Medicine Interview Information 2023 v1Document4 pagesSchool of Medicine Interview Information 2023 v1dovidNo ratings yet
- 2.ORE GuidanceDocument6 pages2.ORE GuidanceMostak Ahmed FaysalNo ratings yet
- Course BookDocument131 pagesCourse Bookimec_coordinator7353100% (1)
- PH Fundamentals AssDocument9 pagesPH Fundamentals AssGkou DojkuNo ratings yet
- Practical Examination Handbook May 2016Document32 pagesPractical Examination Handbook May 2016mandyNo ratings yet
- Practical Examination Handbook 2015Document27 pagesPractical Examination Handbook 2015Neha GurdasaniNo ratings yet
- Final Written English 2013Document10 pagesFinal Written English 2013Jacqueline G GerocheNo ratings yet
- Allied Health Certifications Candidate HB Ver 6.0 FINALDocument17 pagesAllied Health Certifications Candidate HB Ver 6.0 FINALorangegirl002100% (2)
- Dental Ceramics PDFDocument34 pagesDental Ceramics PDFafsal latheefNo ratings yet
- Required Coursework For Dental SchoolDocument5 pagesRequired Coursework For Dental Schoolrqaeibifg100% (2)
- Resume For Dentist in CanadaDocument6 pagesResume For Dentist in Canadac2q5bm7q100% (1)
- Upenn Application Pass - ApplicationDocument2 pagesUpenn Application Pass - ApplicationUshma VyasNo ratings yet
- File 79 PDFDocument159 pagesFile 79 PDFSuzanne Le100% (1)
- Pearson International Certificate Test Taker HandbookDocument17 pagesPearson International Certificate Test Taker HandbookAnnmol JoseNo ratings yet
- Dental Admission Test Frequently Asked Questions: Obtain A DENTPIN and Apply To TestDocument10 pagesDental Admission Test Frequently Asked Questions: Obtain A DENTPIN and Apply To TestNathan Goodson-GreggNo ratings yet
- Well AP Candidate HandbookDocument18 pagesWell AP Candidate HandbookChiara AbbracciodiLuce PolidoroNo ratings yet
- Thesis Statement For Dental AssistantDocument4 pagesThesis Statement For Dental Assistantsandracampbellreno100% (1)
- Las Vegas FormDocument4 pagesLas Vegas FormMohammad ElwirNo ratings yet
- 09 27 Final Draft Well Ap HandbookDocument21 pages09 27 Final Draft Well Ap Handbookjaviera salazarNo ratings yet
- Homes England Graduate Programme Guidance 2024: The Housing and Regeneration AgencyDocument7 pagesHomes England Graduate Programme Guidance 2024: The Housing and Regeneration AgencyMadeline JonesNo ratings yet
- ADEA CAAPID InstructionsDocument10 pagesADEA CAAPID Instructionsshyam05_narainNo ratings yet
- Prometric Exam Information (Y16SYD5219)Document4 pagesPrometric Exam Information (Y16SYD5219)Ali Nawaz AhmedNo ratings yet
- Ielts Faqs Updated On Mar 2016Document10 pagesIelts Faqs Updated On Mar 2016Khan aadil KhaliqNo ratings yet
- Exam Guidance and Instructions: September 2020 ExamsDocument11 pagesExam Guidance and Instructions: September 2020 ExamsNicholas Anthony100% (1)
- Advanced Pest AssDocument46 pagesAdvanced Pest AssGkou DojkuNo ratings yet
- Understanding Results Guide For Students Parents CarersDocument5 pagesUnderstanding Results Guide For Students Parents CarersAisha JananNo ratings yet
- QbyE Hairdressing AgreementDocument6 pagesQbyE Hairdressing AgreementHITONo ratings yet
- Agricultural Pesticide Awareness CEU Training: Registration FormDocument49 pagesAgricultural Pesticide Awareness CEU Training: Registration FormGkou DojkuNo ratings yet
- UoG Placements General Information GuideDocument21 pagesUoG Placements General Information GuideJack ThomsonNo ratings yet
- Dental Hygienist Resume SampleDocument5 pagesDental Hygienist Resume Samplef0jimub1lef2100% (2)
- Spider Control AssDocument45 pagesSpider Control AssGkou DojkuNo ratings yet
- DENTAL AUXILIARY EDUCATION EXAMINATION IN DENTAL MATERIALS: Passbooks Study GuideFrom EverandDENTAL AUXILIARY EDUCATION EXAMINATION IN DENTAL MATERIALS: Passbooks Study GuideNo ratings yet
- Data Center Certified Associate Exam F AqsDocument2 pagesData Center Certified Associate Exam F AqsrihanNo ratings yet
- Florida Real Estate Sales Candidate BookletDocument18 pagesFlorida Real Estate Sales Candidate BookletAzul MezaNo ratings yet
- Psychometric AssessmentDocument9 pagesPsychometric Assessmentbalablooms100% (1)
- Asnt Level 1 Thermography Course ManualDocument45 pagesAsnt Level 1 Thermography Course Manualchitturi jagadish100% (1)
- Ethical Theory For Fraud ExaminersDocument50 pagesEthical Theory For Fraud Examinersveverex100% (2)
- Assessor Training Course For ART Centre Accreditation ProgramDocument7 pagesAssessor Training Course For ART Centre Accreditation ProgramVijay Srishti Fertility Center HosurNo ratings yet
- Optometry Admission Test Frequently Asked Questions: PIN P I NDocument7 pagesOptometry Admission Test Frequently Asked Questions: PIN P I NayanoraNo ratings yet
- How To Write Resume For DentistDocument4 pagesHow To Write Resume For Dentistasbbrfsmd100% (1)
- Thesis Examination BoardDocument4 pagesThesis Examination Boardcrfzqkvcf100% (2)
- Cockroach Control AssDocument137 pagesCockroach Control AssGkou DojkuNo ratings yet
- Ce 45Document1 pageCe 45api-502971487No ratings yet
- Dental Careers of Southflorida: 2011 CatalogDocument18 pagesDental Careers of Southflorida: 2011 Catalogdrhansmann2No ratings yet
- PTE Academic Test Taker Handbook - May 2022 V2Document22 pagesPTE Academic Test Taker Handbook - May 2022 V2Tatiana KabanovaNo ratings yet
- PTE Academic Test Taker Handbook - May 2022 V2Document22 pagesPTE Academic Test Taker Handbook - May 2022 V2MobilaeSoftNo ratings yet
- PTE Academic Test Taker Handbook - May 2022 V2Document22 pagesPTE Academic Test Taker Handbook - May 2022 V2Tommy Linny H.No ratings yet
- A Step by Step Process of ORE Application 2Document12 pagesA Step by Step Process of ORE Application 2رغد شوكت تايه مسعودNo ratings yet
- Electrician (Automobile): Passbooks Study GuideFrom EverandElectrician (Automobile): Passbooks Study GuideNo ratings yet
- Sant Jarnail Singh Bhindranwale - Life, Mission, and MartyrdomDocument62 pagesSant Jarnail Singh Bhindranwale - Life, Mission, and MartyrdomAmandeep Singh AujlaNo ratings yet
- Sant TukArAm English BiographyDocument16 pagesSant TukArAm English BiographyGanesh RahaneNo ratings yet
- Saints and Mahatmas of IndiaDocument290 pagesSaints and Mahatmas of IndiaRajeswari Ranganathan100% (1)
- TheoreticalExamWithAnswers 2012 PDFDocument50 pagesTheoreticalExamWithAnswers 2012 PDFiugulescu laurentiuNo ratings yet
- Essential Mineral Calcium and Its Role in Bone HealthDocument14 pagesEssential Mineral Calcium and Its Role in Bone HealthHabsah Omar MasrunaNo ratings yet
- Part II Color Oral Pathology Picture Booklet (2007-2008) PDFDocument14 pagesPart II Color Oral Pathology Picture Booklet (2007-2008) PDFaerowongNo ratings yet
- TMP - 2243-Inst. Advt. No. 02 of 2016 - 12 Posts281220077Document51 pagesTMP - 2243-Inst. Advt. No. 02 of 2016 - 12 Posts281220077savyasachinNo ratings yet
- Relevance To Public Health: 2.1 Background and Environmental Exposures To Boron in The United StatesDocument13 pagesRelevance To Public Health: 2.1 Background and Environmental Exposures To Boron in The United StatesKhayrunnisa BMNo ratings yet
- TMP 2243-Instructions For Candidates-1462031165Document7 pagesTMP 2243-Instructions For Candidates-1462031165savyasachinNo ratings yet
- Fluorine NMRDocument35 pagesFluorine NMRDrHamadNo ratings yet
- Food Sources of CalciumDocument4 pagesFood Sources of CalciumsavyasachinNo ratings yet
- VitaminDocument8 pagesVitamindrusmansaleemNo ratings yet
- Dragon Naturally Speaking 10Document1 pageDragon Naturally Speaking 10Norazaliza LizaNo ratings yet
- Nutfluoride PDFDocument12 pagesNutfluoride PDFsavyasachinNo ratings yet
- Uch 015741Document2 pagesUch 015741savyasachinNo ratings yet
- Ppssastri Adiparva Part1Document1,005 pagesPpssastri Adiparva Part1savyasachinNo ratings yet
- Nut FluorideDocument4 pagesNut FluoridesavyasachinNo ratings yet
- Dragon NaturallySpeaking 11Document71 pagesDragon NaturallySpeaking 11savyasachinNo ratings yet
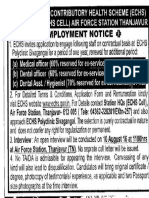
- Ex-Servicemen Contributory Health Scheme (Echs) Jamnagar & Rajkot Employment NoticeDocument1 pageEx-Servicemen Contributory Health Scheme (Echs) Jamnagar & Rajkot Employment NoticesavyasachinNo ratings yet
- ReadMe PDFDocument1 pageReadMe PDFsavyasachinNo ratings yet
- AIIMS PG July 2016 ProspectusDocument56 pagesAIIMS PG July 2016 ProspectussavyasachinNo ratings yet
- ReadMe PDFDocument1 pageReadMe PDFsavyasachinNo ratings yet
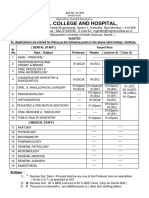
- MGM Dental Coll Navi Mumbai 130214Document2 pagesMGM Dental Coll Navi Mumbai 130214savyasachinNo ratings yet
- Fellowship Revision by Government of IndiaDocument3 pagesFellowship Revision by Government of Indiaatul_saraf001No ratings yet
- ApplicationForm PDFDocument1 pageApplicationForm PDFsavyasachinNo ratings yet
- Prospectus Jan2017Document59 pagesProspectus Jan2017savyasachinNo ratings yet
- Adv PcscoimDocument1 pageAdv PcscoimsavyasachinNo ratings yet
- JRADEDocument2 pagesJRADEsavyasachinNo ratings yet
- Prospectus Jan2017Document59 pagesProspectus Jan2017savyasachinNo ratings yet
- Ex-Servicemen Contributory Health Scheme (Echs) Jamnagar & Rajkot Employment NoticeDocument1 pageEx-Servicemen Contributory Health Scheme (Echs) Jamnagar & Rajkot Employment NoticesavyasachinNo ratings yet