You might also like
- Basic Principles of Wound ManagementDocument14 pagesBasic Principles of Wound ManagementLuis RuizNo ratings yet
- Guidelines On Aesthetic Medical Practice For Registered Medical PractitionersDocument47 pagesGuidelines On Aesthetic Medical Practice For Registered Medical Practitionerszahisma890% (1)
- Management of Analgesia and Sedation in the Polytraumatized patientFrom EverandManagement of Analgesia and Sedation in the Polytraumatized patientNo ratings yet
- Callosities, Corns, and Calluses: BMJ Clinical Research July 1996Document5 pagesCallosities, Corns, and Calluses: BMJ Clinical Research July 1996dewiswahyu100% (1)
- Structural Fat GraftingDocument19 pagesStructural Fat GraftingGautam KalraNo ratings yet
- Bowel Obstruction SurgeryDocument12 pagesBowel Obstruction SurgeryDivya JoyNo ratings yet
- Osteoporosis: Osteoporosis - Devashish Kumar 27701913031 (4th Year, 7 Sem) 27701913031Document12 pagesOsteoporosis: Osteoporosis - Devashish Kumar 27701913031 (4th Year, 7 Sem) 27701913031amish rajNo ratings yet
- Skin Anatomy and PhysiologyDocument5 pagesSkin Anatomy and PhysiologyKhan KamaalNo ratings yet
- PsoriasisDocument40 pagesPsoriasisAmrit Preet KaurNo ratings yet
- Atopic DermatitisDocument26 pagesAtopic DermatitisninarizkiNo ratings yet
- Bacterial Infections of The Skin, Soft TissuesDocument27 pagesBacterial Infections of The Skin, Soft TissuesSHIHAB UDDIN KAZI100% (1)
- OsteomyelitisDocument13 pagesOsteomyelitisKim Enrico JumarangNo ratings yet
- Wound Essentials 8 1 Debridement Consensus Recommendations For PracticeDocument5 pagesWound Essentials 8 1 Debridement Consensus Recommendations For PracticeAndaz MortinNo ratings yet
- Management of Bed SoreDocument19 pagesManagement of Bed Soreugandanursingschool bwindi100% (1)
- Hemorrhoids PresentationDocument24 pagesHemorrhoids PresentationManish upreti100% (1)
- 1.introduction To DermatologyDocument57 pages1.introduction To DermatologyMutasım Battah100% (2)
- Post Op Assessment SurgeryDocument20 pagesPost Op Assessment SurgeryAbdullah MatarNo ratings yet
- Botox For Plantar FasciitisDocument31 pagesBotox For Plantar FasciitisAngie BongNo ratings yet
- Kuliah UKI - Wound HealingDocument32 pagesKuliah UKI - Wound HealingFina Rachma Destafany100% (1)
- Standard Treatment GuidelinesDocument5 pagesStandard Treatment Guidelinesbournvilleeater100% (1)
- Scleroderma - A Case ReportDocument3 pagesScleroderma - A Case Reportdhea nadhiaNo ratings yet
- DRM Policy & StrategyDocument36 pagesDRM Policy & StrategyMarkan GetnetNo ratings yet
- Inflammation and Wound HealingDocument3 pagesInflammation and Wound HealingPrincess AgarwalNo ratings yet
- Perichondritis PinnaDocument2 pagesPerichondritis PinnaAnish RajNo ratings yet
- History of The Suture Personal Suture Preference Suture CharacteristicsDocument33 pagesHistory of The Suture Personal Suture Preference Suture Characteristicsmob3No ratings yet
- LymphomaDocument13 pagesLymphomaRAJKUMARNo ratings yet
- Fracture ManagementDocument21 pagesFracture ManagementPatrickk WandererNo ratings yet
- Wound Management MDocument43 pagesWound Management MMeenuNo ratings yet
- List of Diseases and Its Causative AgentDocument46 pagesList of Diseases and Its Causative AgentPʀɩŋcɘss LɩʌNo ratings yet
- Antifungal Drugs 3Document54 pagesAntifungal Drugs 3Mikee MeladNo ratings yet
- Skin Cancer!Document8 pagesSkin Cancer!HudiansyahNo ratings yet
- Post Op Wound Care Instructions in Clinic For StudentDocument1 pagePost Op Wound Care Instructions in Clinic For StudentrezzkNo ratings yet
- Wound CareDocument5 pagesWound CareEdgar Garcia100% (1)
- BotulismDocument2 pagesBotulismAdrian MangahasNo ratings yet
- Rheumatoid ArthritisDocument20 pagesRheumatoid ArthritisShaibu Ham0% (1)
- Drugs For Osteoarthritis Revise 2010Document65 pagesDrugs For Osteoarthritis Revise 2010Nofilia Citra CandraNo ratings yet
- Melanoma CaseDocument4 pagesMelanoma CaseDinarkram Rabreca EculNo ratings yet
- ConjunctivitisDocument26 pagesConjunctivitisNikki M. ArapolNo ratings yet
- EndocrinologyDocument23 pagesEndocrinologysaikat55No ratings yet
- Diagnosis Treatment of Back Pain MedicationsDocument41 pagesDiagnosis Treatment of Back Pain Medicationsrabin1994No ratings yet
- NHO Medical Abbreviations BookletDocument54 pagesNHO Medical Abbreviations BookletffsdfsfdftrertNo ratings yet
- Systemic Lupus ErythematosusDocument16 pagesSystemic Lupus ErythematosusSaharNo ratings yet
- Uses of Surgical InstrumentsDocument10 pagesUses of Surgical InstrumentsjaidinjdNo ratings yet
- Short Wave DiathermyDocument73 pagesShort Wave DiathermySabarie PNo ratings yet
- Burns: James Taclin C. Banez M.D., FPSGS, FPCSDocument48 pagesBurns: James Taclin C. Banez M.D., FPSGS, FPCSCodillia CheongNo ratings yet
- Risk Factors of Gastritis and Its Prevalence Among Patients Visiting Kalkaal Hospital, Mogadishu, SomaliaDocument6 pagesRisk Factors of Gastritis and Its Prevalence Among Patients Visiting Kalkaal Hospital, Mogadishu, SomaliaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Arthritis: Group 6Document24 pagesArthritis: Group 6Jenneth Marquez JoloNo ratings yet
- Burns: Major and Minor BurnsDocument25 pagesBurns: Major and Minor BurnsTrisha TannerNo ratings yet
- Wound Care, Dressing and BandagingDocument11 pagesWound Care, Dressing and BandagingJessica Febrina Wuisan100% (1)
- Sutures: Dr. Oyebode OyeyiolaDocument50 pagesSutures: Dr. Oyebode Oyeyiolaoyebode oyeyiolaNo ratings yet
- Wounds & Wound HealingDocument47 pagesWounds & Wound HealingDrSarmad100% (3)
- Alopecia: By. Mr. P. Dhilip KumarDocument9 pagesAlopecia: By. Mr. P. Dhilip Kumarpreet kaur100% (1)
- Psoriatic ArthritisDocument12 pagesPsoriatic ArthritisSelvia RosadiNo ratings yet
- Laboratory Diagnosis of Wounds InfectionsDocument15 pagesLaboratory Diagnosis of Wounds Infectionsanum100% (1)
- Transferring People Safely - WebDocument36 pagesTransferring People Safely - Webkimbakicks100% (1)
- Pressure Ulcer CareDocument39 pagesPressure Ulcer CareRosalyn YuNo ratings yet
- Medical AbbreviationsDocument21 pagesMedical AbbreviationsReachel Ann RonquilloNo ratings yet
- Medical Application For LASERDocument3 pagesMedical Application For LASERAnonymous xzi9LiT100% (1)
- Jurnal AnastesiDocument16 pagesJurnal AnastesiHanarisha Putri AzkiaNo ratings yet
- SMF Anak Rsud Jend. A. Yani Metro Kepaniteraan Klinik FK Unila 2017Document1 pageSMF Anak Rsud Jend. A. Yani Metro Kepaniteraan Klinik FK Unila 2017Hanarisha Putri AzkiaNo ratings yet
- Icu Kidney Injury AcuteDocument7 pagesIcu Kidney Injury AcuteHanarisha Putri AzkiaNo ratings yet
- DM Foot CareDocument27 pagesDM Foot CareKatrina KattNo ratings yet
- Colorectal Cancer, How To Diagnosis and TherapyDocument33 pagesColorectal Cancer, How To Diagnosis and TherapyHanarisha Putri AzkiaNo ratings yet
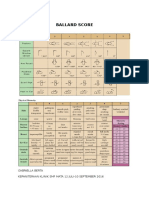
- Ballard Score: Gabriella Berta Kepaniteraan Klinik SMF Mata 12 Juli-10 September 2016Document1 pageBallard Score: Gabriella Berta Kepaniteraan Klinik SMF Mata 12 Juli-10 September 2016Hanarisha Putri AzkiaNo ratings yet
- Burns Management PDFDocument7 pagesBurns Management PDFRoh Bungaria N Garingging100% (1)
- 2.5 Assesment of Diabetic Foot UlcerDocument10 pages2.5 Assesment of Diabetic Foot UlcerHanarisha Putri AzkiaNo ratings yet
- IUGR New Concepts - AJOG ReviewDocument13 pagesIUGR New Concepts - AJOG ReviewHanarisha Putri AzkiaNo ratings yet
- Asymptomatic Bacteriuria in Adults: (E.g., P. Aeruginosa) - Enterococcus Species andDocument6 pagesAsymptomatic Bacteriuria in Adults: (E.g., P. Aeruginosa) - Enterococcus Species andHanarisha Putri AzkiaNo ratings yet
- Journal ReadingDocument11 pagesJournal ReadingHanarisha Putri AzkiaNo ratings yet
- Tropical AlmondDocument9 pagesTropical AlmondHanarisha Putri AzkiaNo ratings yet
- Burn Patient Management - Clinical Practice GuidelinesDocument47 pagesBurn Patient Management - Clinical Practice GuidelinesAna PNo ratings yet
- Faktor Dominan Yang Berhubungan Dengan Kejadian Abortus Imminens Hamidah, Siti MasitohDocument1 pageFaktor Dominan Yang Berhubungan Dengan Kejadian Abortus Imminens Hamidah, Siti MasitohHanarisha Putri AzkiaNo ratings yet
- Daftar Pustaka RefDocument3 pagesDaftar Pustaka RefHanarisha Putri AzkiaNo ratings yet
- Burns Management PDFDocument7 pagesBurns Management PDFRoh Bungaria N Garingging100% (1)
- Burn Patient Management - Clinical Practice GuidelinesDocument47 pagesBurn Patient Management - Clinical Practice GuidelinesAna PNo ratings yet
- Anencephaly: A 3 Years Study: DR - Aruna.Eslavath (MD), Dr. Ranga Rao - Diddi (MD), DR - Kalyan Chakravarthy - Valabhaneni (MD)Document4 pagesAnencephaly: A 3 Years Study: DR - Aruna.Eslavath (MD), Dr. Ranga Rao - Diddi (MD), DR - Kalyan Chakravarthy - Valabhaneni (MD)Hanarisha Putri AzkiaNo ratings yet
- Dapus BaruDocument1 pageDapus BaruHanarisha Putri AzkiaNo ratings yet
- ABCs Skin and Wound CareDocument2 pagesABCs Skin and Wound CareHanarisha Putri AzkiaNo ratings yet
- Neural Tube Defects - Anencephaly - HP - FASP76Document5 pagesNeural Tube Defects - Anencephaly - HP - FASP76Hanarisha Putri AzkiaNo ratings yet
- Reduction in NTD in CanadaDocument8 pagesReduction in NTD in CanadaHanarisha Putri AzkiaNo ratings yet
- CFT Terminalia CatappaDocument2 pagesCFT Terminalia CatappaHanarisha Putri AzkiaNo ratings yet
- Am. J. Epidemiol. 2005 Boyko 557 64Document8 pagesAm. J. Epidemiol. 2005 Boyko 557 64Hanarisha Putri AzkiaNo ratings yet
- Pmed 1000367Document9 pagesPmed 1000367Hanarisha Putri AzkiaNo ratings yet
- Journal of Diagnostic Medical Sonography 2010 Moore 286 9Document4 pagesJournal of Diagnostic Medical Sonography 2010 Moore 286 9Hanarisha Putri AzkiaNo ratings yet
- Types of WoundsDocument4 pagesTypes of WoundsHanarisha Putri AzkiaNo ratings yet
- Bates-Jensen Wound Assessment Tool (BWAT)Document4 pagesBates-Jensen Wound Assessment Tool (BWAT)Jamie OngNo ratings yet
- Asymptomatic BacteriuriaDocument12 pagesAsymptomatic BacteriuriaNanna de VengerbergNo ratings yet
- HomeostasisDocument8 pagesHomeostasisLely SharmaNo ratings yet
- PHD Admission Brochure: Department of Chemical EngineeringDocument10 pagesPHD Admission Brochure: Department of Chemical EngineeringVijaykumar JatothNo ratings yet
- Blood Is The "River of Life" That Surges Within UsDocument16 pagesBlood Is The "River of Life" That Surges Within UsKyle LumingkitNo ratings yet
- Best of Five Mcqs For The Gastroenterology Sce PDFDocument315 pagesBest of Five Mcqs For The Gastroenterology Sce PDFSabry Anees100% (8)
- Blood Transfusion LearningDocument36 pagesBlood Transfusion LearningHarjotBrarNo ratings yet
- Nursing Care Plan For HELLP SyndromeDocument17 pagesNursing Care Plan For HELLP SyndromeRosemarie Carpio75% (4)
- Vit K Drug StudyDocument2 pagesVit K Drug StudyTrina Joy Domantay100% (1)
- Anticoagulant Mcqs ExplainedDocument3 pagesAnticoagulant Mcqs ExplainedHawi BefekaduNo ratings yet
- Plasma FractionationDocument40 pagesPlasma FractionationJoseph ChandyNo ratings yet
- Pathophysiology of SepsisDocument7 pagesPathophysiology of SepsisUntuk DownloadNo ratings yet
- Biology: Pearson Edexcel GCEDocument183 pagesBiology: Pearson Edexcel GCEaliceNo ratings yet
- Packing ReviewDocument16 pagesPacking ReviewChandrasekaryas2010No ratings yet
- Chapter 30: Hematologic Disorders Linton: Medical-Surgical Nursing, 7th EditionDocument5 pagesChapter 30: Hematologic Disorders Linton: Medical-Surgical Nursing, 7th EditionStaceyNo ratings yet
- MSDS AsparginaseDocument9 pagesMSDS AsparginaseClarissa AdhyatmanNo ratings yet
- Ijcpd-15-S103 MetanalysisDocument11 pagesIjcpd-15-S103 MetanalysisGabriela ZuritaNo ratings yet
- Valpros PediaDocument2 pagesValpros PediaAnnsh Hadji EliasNo ratings yet
- SF 8050 enDocument2 pagesSF 8050 enNghi NguyenNo ratings yet
- Survey of Ethno Medicinal Plant Showing Wound Healing ActivityDocument18 pagesSurvey of Ethno Medicinal Plant Showing Wound Healing ActivityIJAR JOURNALNo ratings yet
- Burn Injury and Blood Transfusion: ReviewDocument5 pagesBurn Injury and Blood Transfusion: Reviewasadad adsdasasdadNo ratings yet
- Composition and Functions: BloodDocument86 pagesComposition and Functions: BloodYeyeh SantosNo ratings yet
- Hematologic DisorderDocument7 pagesHematologic Disordermawel100% (2)
- 1 - Introduction To HematologyDocument38 pages1 - Introduction To HematologyMelanie Tran100% (1)
- AnticoagulantsDocument47 pagesAnticoagulantsMARK VINCENT BAUTISTANo ratings yet
- DCI GeneralDocument148 pagesDCI GeneralMemo UNNo ratings yet
- Bleeding Disorders in Ortho PDFDocument4 pagesBleeding Disorders in Ortho PDFkiran kaurNo ratings yet
- Tranaxemic AcidDocument6 pagesTranaxemic AcidCharan Teja ReddyNo ratings yet
- Using Enzymes To Diagnose DiseasesDocument30 pagesUsing Enzymes To Diagnose DiseasesAnubhav sainiNo ratings yet
- Artikel Ie Asam SuntiDocument5 pagesArtikel Ie Asam SuntiHarzukilNo ratings yet
- New Oral Anticoagulants For Stroke Prevention in Atrial FibrillationDocument1 pageNew Oral Anticoagulants For Stroke Prevention in Atrial FibrillationmngalaxyNo ratings yet
- Screenshot 2023-12-11 at 3.53.36 PMDocument62 pagesScreenshot 2023-12-11 at 3.53.36 PMahmedmansi055No ratings yet
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (2)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (28)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (81)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (393)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)No ratings yet
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (4)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Marshmallow Test: Mastering Self-ControlFrom EverandThe Marshmallow Test: Mastering Self-ControlRating: 4.5 out of 5 stars4.5/5 (58)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (170)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingFrom EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingRating: 4 out of 5 stars4/5 (1138)