You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- LWS101 Week 2 Ethics PPTslidesDocument44 pagesLWS101 Week 2 Ethics PPTslidesJanet YauNo ratings yet
- Hordeolum - Background, Pathophysiology, EpidemiologyDocument6 pagesHordeolum - Background, Pathophysiology, EpidemiologyKeren SingamNo ratings yet
- Medical Application FormDocument5 pagesMedical Application FormRaz De NeiNo ratings yet
- Movement DisordersDocument18 pagesMovement DisordersFaisal BudisasmitaNo ratings yet
- Therapeutic Drug MonitoringDocument6 pagesTherapeutic Drug MonitoringEdi Uchiha SutarmantoNo ratings yet
- Post Anaesthesia Shivering - N PadayacheeDocument19 pagesPost Anaesthesia Shivering - N Padayacheexxxvrgnt100% (2)
- SchizophreniaDocument67 pagesSchizophreniaHazirah Mokhtar100% (1)
- Rca - Lauren HerrDocument5 pagesRca - Lauren Herrapi-520453750No ratings yet
- What Is The Appendix?: Symptoms of AppendicitisDocument6 pagesWhat Is The Appendix?: Symptoms of AppendicitisVonn Bryan CalumiaNo ratings yet
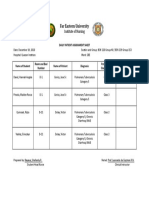
- Daily Patient Assignment SheetDocument1 pageDaily Patient Assignment SheetSheferely BayauaNo ratings yet
- Hat User ManualDocument10 pagesHat User ManualIRAWANNo ratings yet
- Resume Nurse InformaticistDocument2 pagesResume Nurse Informaticistapi-655449085No ratings yet
- Text CDocument1,100 pagesText CAli NofalNo ratings yet
- Endoscopic Skull Base SurgeryDocument25 pagesEndoscopic Skull Base Surgerypramod454992No ratings yet
- Agglutination ReactionsDocument28 pagesAgglutination ReactionscyrhenmieNo ratings yet
- English Communication For Healthcare Service: Topic 2: FamilyDocument5 pagesEnglish Communication For Healthcare Service: Topic 2: FamilyBảoNgọcNo ratings yet
- Procedure For Insertion of Saf T Intima Cannula and Subcutaneous InjectionDocument16 pagesProcedure For Insertion of Saf T Intima Cannula and Subcutaneous Injectionmadimadi11No ratings yet
- Renzo Colombo, Richard Naspro PDFDocument9 pagesRenzo Colombo, Richard Naspro PDFHidayah Mararotua HarahapNo ratings yet
- USPI-Zithromax - Azithromycin - IVDocument22 pagesUSPI-Zithromax - Azithromycin - IVTufail AhmedNo ratings yet
- DPRG FallNewsletter2013Document8 pagesDPRG FallNewsletter2013RichieDaisyNo ratings yet
- Antihyperglycemic Agents Comparison ChartDocument9 pagesAntihyperglycemic Agents Comparison ChartBonnieNo ratings yet
- Ms 1Document3 pagesMs 1Rachelle Jillian LegaspiNo ratings yet
- Diabetes QuestionsDocument6 pagesDiabetes QuestionsLara B100% (3)
- Regional Sales Manager Medical Devices in Dallas FT Worth TX Resume James MooreDocument2 pagesRegional Sales Manager Medical Devices in Dallas FT Worth TX Resume James MooreJamesMoore2No ratings yet
- Kep KritisDocument193 pagesKep Kritisari cahyaNo ratings yet
- Hip Pain TreatmentDocument19 pagesHip Pain TreatmentLev KalikaNo ratings yet
- 3d66 PDFDocument60 pages3d66 PDFAnindya EvanNo ratings yet
- Keefe. The Schizophrenia Cognition Rating ScaleDocument7 pagesKeefe. The Schizophrenia Cognition Rating ScaleRosarioBengocheaSeco0% (1)
- EMS CatalogDocument25 pagesEMS Catalogrrockel100% (1)
- Alteration in Family ProcessesDocument2 pagesAlteration in Family ProcessesCatherine Cayda dela Cruz-BenjaminNo ratings yet