You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Advt of Nursing Officer For 4 AIIMS - 1Document10 pagesAdvt of Nursing Officer For 4 AIIMS - 1prashanthNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- 2TIME TABLE - 2013 Batch Third YearDocument2 pages2TIME TABLE - 2013 Batch Third YearprashanthNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Addendum For PWBD For Online RegDocument1 pageAddendum For PWBD For Online Regprashanth100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Notice Result Extend - NursingOfficer - 2019Document1 pageNotice Result Extend - NursingOfficer - 2019prashanthNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- 2TIME TABLE - 2013 Batch Third YearDocument2 pages2TIME TABLE - 2013 Batch Third YearprashanthNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- United India Insurance Recruitment for 300+ VacanciesDocument29 pagesUnited India Insurance Recruitment for 300+ VacanciesRavi SrivastavaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Cghs Nabh Application HospitalDocument27 pagesCghs Nabh Application HospitalGaurav SharmaNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Final Result - Nursing Officer Central Hospitals-2019-NETDocument17 pagesFinal Result - Nursing Officer Central Hospitals-2019-NETprashanthNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Medical MalpracticeDocument41 pagesMedical MalpracticeprashanthNo ratings yet
- Your Bibliography VancouverDocument1 pageYour Bibliography VancouverprashanthNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
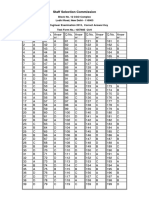
- SSC JE 2015 Exam Correct Answer Key for Test Form 1057685Document2 pagesSSC JE 2015 Exam Correct Answer Key for Test Form 1057685prashanthNo ratings yet
- M.O.S.C.College of Nursing 3 Year BSC Nursing Pattern of ExaminationDocument1 pageM.O.S.C.College of Nursing 3 Year BSC Nursing Pattern of ExaminationprashanthNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- HMIS Kerala RevisedDocument34 pagesHMIS Kerala RevisedprashanthNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Project ReportDocument2 pagesProject ReportprashanthNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Post Basic BSC Admn PlanDocument2 pagesPost Basic BSC Admn PlanprashanthNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- M.O.S.C.College of Nursing, Kolenchery 3Rd Year B.Sc. Nursing Degree Course (2013-17 Batch) Clinical PlanDocument12 pagesM.O.S.C.College of Nursing, Kolenchery 3Rd Year B.Sc. Nursing Degree Course (2013-17 Batch) Clinical PlanprashanthNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Seminar On BUDGETDocument14 pagesSeminar On BUDGETprashanth60% (5)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- Martha RogerDocument10 pagesMartha RogerprashanthNo ratings yet
- Physical ExaminationDocument39 pagesPhysical ExaminationprashanthNo ratings yet
- Diabetic Foot Care OverviewDocument21 pagesDiabetic Foot Care Overviewprashanth100% (4)
- 8TIME TABLE - 2013 Batch Third YearDocument2 pages8TIME TABLE - 2013 Batch Third YearprashanthNo ratings yet
- OremDocument12 pagesOremprashanthNo ratings yet
- Calculation of Clinical HoursDocument1 pageCalculation of Clinical HoursprashanthNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Bowel IncontinenceDocument4 pagesBowel IncontinenceprashanthNo ratings yet
- ANP Clinical Rotation 2015 SinuDocument4 pagesANP Clinical Rotation 2015 SinuprashanthNo ratings yet
- M.O.S.C College of Nursing Kolenchery: Anecdotal RecordDocument5 pagesM.O.S.C College of Nursing Kolenchery: Anecdotal RecordprashanthNo ratings yet
- M.O.S.C College Psychiatric Nursing FormsDocument5 pagesM.O.S.C College Psychiatric Nursing FormsprashanthNo ratings yet
- Assessment Format Mental Health NursingDocument11 pagesAssessment Format Mental Health Nursingprashanth100% (1)
- Unit Plan Mental Health NursingDocument2 pagesUnit Plan Mental Health Nursingprashanth100% (2)
- 1 s2.0 S0975947621001923 MainDocument8 pages1 s2.0 S0975947621001923 Mainaman babuNo ratings yet
- PSP TablesDocument32 pagesPSP TablesLucas Cariño LlaconaNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Rorschach y SuicidioDocument17 pagesRorschach y SuicidioLaura SierraNo ratings yet
- Curtain WallDocument11 pagesCurtain WallZameer AhmedNo ratings yet
- JP - Health and Wholeness Through The Holy CommunionDocument62 pagesJP - Health and Wholeness Through The Holy Communionjevontan90% (10)
- Science 6-Q1-M6Document14 pagesScience 6-Q1-M6John Philip LegaspiNo ratings yet
- Colours of the RainbowDocument16 pagesColours of the RainbowMd A RAZZAKNo ratings yet
- Penicillin G Benzathine-Drug StudyDocument2 pagesPenicillin G Benzathine-Drug StudyDaisy Palisoc67% (3)
- embragues-INTORK KBK14800 Erhsa2013 PDFDocument56 pagesembragues-INTORK KBK14800 Erhsa2013 PDFPablo RuizNo ratings yet
- List of Personnel Benefits Granted by The SchoolDocument8 pagesList of Personnel Benefits Granted by The SchoolAspci Assumption Passi100% (1)
- B-64483EN-2 - 05 - 01 Dual Check Safety - CONNECTION MANUAL - Password - RemovedDocument270 pagesB-64483EN-2 - 05 - 01 Dual Check Safety - CONNECTION MANUAL - Password - Removedretox9000No ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- TLC Analysis of Siling Labuyo Extract ComponentsDocument3 pagesTLC Analysis of Siling Labuyo Extract ComponentsJan Eric Balete0% (1)
- Food Regulations MalaysiaDocument4 pagesFood Regulations MalaysiaSyafi'ie Syukri100% (1)
- Effects of Limited Face-to-Face Classes on Grade 11 TVL Students and TeachersDocument45 pagesEffects of Limited Face-to-Face Classes on Grade 11 TVL Students and TeachersJoseph Xyrel Malacad100% (1)
- HZB-15S Service ManualDocument20 pagesHZB-15S Service ManualJason Cravy100% (1)
- Archives of Oral Biology 100 (2019) 42-48Document7 pagesArchives of Oral Biology 100 (2019) 42-48pedro cuellar proNo ratings yet
- Fundamentals of Plant BreedingDocument190 pagesFundamentals of Plant BreedingDave SubiyantoNo ratings yet
- Common Safety Method GuidanceDocument66 pagesCommon Safety Method GuidanceDiego UngerNo ratings yet
- 310 Ta PDFDocument8 pages310 Ta PDFVincent GomuliaNo ratings yet
- SinogramDocument2 pagesSinogramNguyễn Thành CôngNo ratings yet
- Structure Dismantling JSADocument2 pagesStructure Dismantling JSAtnssbhaskar69% (13)
- Review of Literature Review of LiteratureDocument31 pagesReview of Literature Review of LiteratureeswariNo ratings yet
- Manual Murray 20Document28 pagesManual Murray 20freebanker777741No ratings yet
- Coca Cola Primary Activities: 1. Inbound Logistics Include Functions Like Receiving, Warehousing, and Managing InventoryDocument5 pagesCoca Cola Primary Activities: 1. Inbound Logistics Include Functions Like Receiving, Warehousing, and Managing InventoryJaene L.No ratings yet
- A Comparative Study Between Various Models of Eco-Brick and Hollow BlocksDocument9 pagesA Comparative Study Between Various Models of Eco-Brick and Hollow BlocksMykaila Ysa ValdezNo ratings yet
- QS - HM - Freight Express Indonesia - Cipta HarapanDocument4 pagesQS - HM - Freight Express Indonesia - Cipta HarapanAKHMAD SHOQI ALBINo ratings yet
- KPI and Supplier Performance Scorecard ToolDocument7 pagesKPI and Supplier Performance Scorecard ToolJayant Kumar JhaNo ratings yet
- Muis Kidney Book ENGDocument17 pagesMuis Kidney Book ENGCrystyan CryssNo ratings yet
- Preparation of Salts (Multiple Choice) QPDocument8 pagesPreparation of Salts (Multiple Choice) QPkhalil rehmanNo ratings yet
- Arthropods: A Guide to the Diverse PhylumDocument10 pagesArthropods: A Guide to the Diverse Phylumpkkalai112No ratings yet
- Maktub: An Inspirational Companion to The AlchemistFrom EverandMaktub: An Inspirational Companion to The AlchemistRating: 5 out of 5 stars5/5 (2)
- When You're Ready, This Is How You HealFrom EverandWhen You're Ready, This Is How You HealRating: 4.5 out of 5 stars4.5/5 (181)
- Permission to Be Gentle: 7 Self-Love Affirmations for the Highly SensitiveFrom EverandPermission to Be Gentle: 7 Self-Love Affirmations for the Highly SensitiveRating: 4.5 out of 5 stars4.5/5 (13)
- The 7 Habits of Highly Effective People: The Infographics EditionFrom EverandThe 7 Habits of Highly Effective People: The Infographics EditionRating: 4 out of 5 stars4/5 (2475)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Summary: Atomic Habits by James Clear: An Easy & Proven Way to Build Good Habits & Break Bad OnesFrom EverandSummary: Atomic Habits by James Clear: An Easy & Proven Way to Build Good Habits & Break Bad OnesRating: 5 out of 5 stars5/5 (1631)