You might also like
- Literatur 2Document7 pagesLiteratur 2aninuraniyahNo ratings yet
- Holstein Hargreaves Endo Topics 2003Document11 pagesHolstein Hargreaves Endo Topics 2003aninuraniyahNo ratings yet
- Holstein Hargreaves Endo Topics 2003Document11 pagesHolstein Hargreaves Endo Topics 2003aninuraniyahNo ratings yet
- Journal ReadingDocument4 pagesJournal ReadingVeny AlfianiNo ratings yet
- 4 PDFDocument3 pages4 PDFLanggeng Perdhana Jangan MenyerahNo ratings yet
- MucoceleDocument4 pagesMucoceleaninuraniyahNo ratings yet
- Restoring Endodontically Treated TeethDocument20 pagesRestoring Endodontically Treated Teethlishenwong100% (1)
- Treated ExfoliativeDocument3 pagesTreated ExfoliativeaninuraniyahNo ratings yet
- Journal ReadingDocument4 pagesJournal ReadingVeny AlfianiNo ratings yet
- MucoceleDocument4 pagesMucoceleaninuraniyahNo ratings yet
- Systemic Diseases Caused by Oral InfectionDocument12 pagesSystemic Diseases Caused by Oral InfectionaninuraniyahNo ratings yet
- 4 PDFDocument3 pages4 PDFLanggeng Perdhana Jangan MenyerahNo ratings yet
- MucoceleDocument4 pagesMucoceleaninuraniyahNo ratings yet
- ExfoliativeDocument4 pagesExfoliativeaninuraniyahNo ratings yet
- Hand Hygiene GuideDocument2 pagesHand Hygiene GuideaninuraniyahNo ratings yet
- Eugenol 3Document7 pagesEugenol 3aninuraniyahNo ratings yet
- Nursing Caries PedoDocument37 pagesNursing Caries PedoFourthMolar.comNo ratings yet
- Gambaran Status KariesDocument9 pagesGambaran Status KariesaninuraniyahNo ratings yet
- EugenolDocument6 pagesEugenolaninuraniyahNo ratings yet
- Clinical tips for full veneer tooth preparationDocument7 pagesClinical tips for full veneer tooth preparationaninuraniyahNo ratings yet
- 90507414Document5 pages90507414aninuraniyahNo ratings yet
- Ranula and Sublingual Salivary Gland ExcisionDocument4 pagesRanula and Sublingual Salivary Gland ExcisionaninuraniyahNo ratings yet
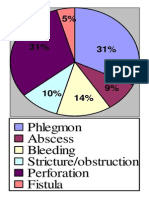
- Phlegmon Abscess Bleeding Stricture/obstruction Perforation FistulaDocument1 pagePhlegmon Abscess Bleeding Stricture/obstruction Perforation FistulaaninuraniyahNo ratings yet
- Eugenol 2Document6 pagesEugenol 2aninuraniyahNo ratings yet
- SterilisasiDocument6 pagesSterilisasianinuraniyahNo ratings yet
- 5-Surgical Treatment of RanulaDocument5 pages5-Surgical Treatment of RanulaDevi AlfianiNo ratings yet
- Jop 2012 110716Document8 pagesJop 2012 110716aninuraniyahNo ratings yet
- Hand Hygiene GuideDocument2 pagesHand Hygiene GuideaninuraniyahNo ratings yet
- Micro-Marsupialization Technique For Mucocele On Ventral Tongue in 4-Year-8-Month Old ChildDocument2 pagesMicro-Marsupialization Technique For Mucocele On Ventral Tongue in 4-Year-8-Month Old ChildaninuraniyahNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Erosion Tecnalia 2016 06Document17 pagesErosion Tecnalia 2016 06FernanNo ratings yet
- EN FM Flammable GeneralDocument2 pagesEN FM Flammable GeneralYedersonNo ratings yet
- Presentation On Forged Mill Balls Production in South AfricaDocument23 pagesPresentation On Forged Mill Balls Production in South AfricaRamoutar (Ken) SeecharranNo ratings yet
- Thermal Analysis of Electrical Machines Limits and Heat Transfer PrinciplesDocument2 pagesThermal Analysis of Electrical Machines Limits and Heat Transfer PrinciplesAnonymous sAmJfcVNo ratings yet
- Low Temperature Behavior of Metals: Fracture Toughness and Ductile to Brittle TransitionDocument39 pagesLow Temperature Behavior of Metals: Fracture Toughness and Ductile to Brittle TransitionkoontattNo ratings yet
- Composite MaterialsDocument399 pagesComposite MaterialsCharlton S.Inao100% (1)
- Tamseal Admix: Description Technical DataDocument2 pagesTamseal Admix: Description Technical DataJoyce Agustine Glory LNo ratings yet
- Bollhoff HeliCoil Plus ImperialDocument48 pagesBollhoff HeliCoil Plus ImperialAce Industrial SuppliesNo ratings yet
- Empirical and Molecular Formulas ExplainedDocument16 pagesEmpirical and Molecular Formulas ExplainedangelaNo ratings yet
- Microwave, IR, NMR spectroscopy techniquesDocument1 pageMicrowave, IR, NMR spectroscopy techniquesSaikiranNo ratings yet
- Indirect RestorationsDocument32 pagesIndirect RestorationsNaji Z. Arandi100% (1)
- EndocrineDocument3 pagesEndocrinePotato HeadNo ratings yet
- LCP SpanlockDocument8 pagesLCP SpanlockGarfieldNo ratings yet
- Physical Properties of SolutionDocument3 pagesPhysical Properties of SolutionRhye Tabaday LopezNo ratings yet
- Bricks PDFDocument86 pagesBricks PDFSai DasaradharamNo ratings yet
- Effect of Preparation Method of Ni Catalyst Using Bentonite As The Support MaterialDocument8 pagesEffect of Preparation Method of Ni Catalyst Using Bentonite As The Support MaterialNastitiNo ratings yet
- Alimentos Funcionais em UanDocument12 pagesAlimentos Funcionais em UanEduardo MartinsNo ratings yet
- Maintain Your BRH 501 Demolition HammerDocument46 pagesMaintain Your BRH 501 Demolition HammerRomán Arturo Guerrero Uc100% (3)
- DPP 20220411175616686155Document52 pagesDPP 20220411175616686155Ronit NigamNo ratings yet
- Depth Filter Sheets: BegerowDocument23 pagesDepth Filter Sheets: BegerowKHUSH PATELNo ratings yet
- Thermal Conductivity Meter: Guarded Heat Flow Test MethodDocument2 pagesThermal Conductivity Meter: Guarded Heat Flow Test Methodrajesh_rbpNo ratings yet
- Sistem Pelumasan: - ReviewDocument72 pagesSistem Pelumasan: - ReviewUncle MTANo ratings yet
- Ductulator May 2010Document8 pagesDuctulator May 2010haroub_nasNo ratings yet
- Lab Manual 11 Infrared SpectrosDocument5 pagesLab Manual 11 Infrared SpectrosLuca Selva CampobassoNo ratings yet
- Research Paper March 10 2019Document12 pagesResearch Paper March 10 2019vincent jancarlo ricarteNo ratings yet
- Chapter 8Document44 pagesChapter 8Oscar Espinosa BonillaNo ratings yet
- LubKlear Brochure LubLineDocument2 pagesLubKlear Brochure LubLineMarcela FariasNo ratings yet
- RocksDocument5 pagesRocksangelic dailyNo ratings yet
- Grammar Files b2 Unit 1Document7 pagesGrammar Files b2 Unit 1Irina Shopova100% (1)
- Int Esws at Y9 Workbook Answers TTPPDocument37 pagesInt Esws at Y9 Workbook Answers TTPPChrystal GraceNo ratings yet