You might also like
- FEHM Final June 2016Document96 pagesFEHM Final June 2016Fatchur RizalNo ratings yet
- Iso22000 2005Document48 pagesIso22000 2005STELLA MARISNo ratings yet
- Questions For Root Cause Analysis Participants (Job Titles)Document4 pagesQuestions For Root Cause Analysis Participants (Job Titles)paul_aldNo ratings yet
- 2013 SHDocument88 pages2013 SHeastNo ratings yet
- 5 Critical Factors RCFADocument22 pages5 Critical Factors RCFAKasinathan MuniandiNo ratings yet
- 96 14saDocument233 pages96 14saiomerko100% (1)
- Lead AuditorDocument1 pageLead Auditorsaravanan ssNo ratings yet
- En - 02. Introduction To RCA MethodologyDocument17 pagesEn - 02. Introduction To RCA MethodologyAlex Palomino DiazNo ratings yet
- The Basics of Disaster ResponseDocument100 pagesThe Basics of Disaster Responseমোঃ সাইদুর রহিম100% (1)
- SmartPlant Enterpise Owner Operator - Process Safety Management and Asset Integrity Management - PertaminaDocument40 pagesSmartPlant Enterpise Owner Operator - Process Safety Management and Asset Integrity Management - PertaminaSilvanaNo ratings yet
- OMS RequirementsDocument16 pagesOMS RequirementsSajith Kottila VeettilNo ratings yet
- Human Factor in OSH-1Document110 pagesHuman Factor in OSH-1Hisham Ismail100% (1)
- Seminar Objectives: Offshore Facility Process Safety OverviewDocument11 pagesSeminar Objectives: Offshore Facility Process Safety OverviewCarlos Domingo Roland CheekNo ratings yet
- How To Achieve Zero AccidentDocument108 pagesHow To Achieve Zero AccidentAjit BhosaleNo ratings yet
- MocDocument45 pagesMoclokhandeatul1100% (2)
- Safety Performance Based On Iogp PDFDocument152 pagesSafety Performance Based On Iogp PDFAJMNo ratings yet
- RAID Register - SapphireDocument11 pagesRAID Register - SapphireMuhammadMuzammalJamilNo ratings yet
- PPI Rig Audit CheckDocument5 pagesPPI Rig Audit CheckAHMED BAKRNo ratings yet
- Daily Progress Report HSE: Date 17/9/18 Equipments UsedDocument1 pageDaily Progress Report HSE: Date 17/9/18 Equipments Usedjithin shankarNo ratings yet
- 1 Wpse Guide PDFDocument74 pages1 Wpse Guide PDFEmmanuel BilfredNo ratings yet
- Incident InvestigationDocument36 pagesIncident InvestigationudbarryNo ratings yet
- FMECA Guide for System Failure AnalysisDocument56 pagesFMECA Guide for System Failure AnalysisYagna VeryNo ratings yet
- Controlling Risks Risk AssessmentDocument23 pagesControlling Risks Risk AssessmentZenitha AmadangiNo ratings yet
- OpitoDocument34 pagesOpitohidayatu solihinNo ratings yet
- Failure Analysis: Key Concepts and Benefits of FMECADocument72 pagesFailure Analysis: Key Concepts and Benefits of FMECAbrucemartin3100% (1)
- Guide To Opito Approval For Training ProvidersDocument31 pagesGuide To Opito Approval For Training ProvidersmashanghNo ratings yet
- FMEA BoilerDocument2 pagesFMEA BoilerKevin FloresNo ratings yet
- Oil and Gas Development Company 2Document4 pagesOil and Gas Development Company 2muhammad farhanNo ratings yet
- A Method For Barrier-Based Incident InvestigationDocument7 pagesA Method For Barrier-Based Incident InvestigationEzatollah SalaryNo ratings yet
- Process Safety Events-2011 & 2012 DataDocument28 pagesProcess Safety Events-2011 & 2012 DataRichard BaileyNo ratings yet
- Introduction to FBD and FTA for Equipment Failure AnalysisDocument12 pagesIntroduction to FBD and FTA for Equipment Failure AnalysisFazli FadzilNo ratings yet
- OIMSDocument20 pagesOIMSWArya RaWigunanNo ratings yet
- For The Health of Your BusinessDocument14 pagesFor The Health of Your BusinessMauricio Santana0% (1)
- Corrective Actions Preventive ActionsDocument33 pagesCorrective Actions Preventive ActionsVidya100% (1)
- 10 Industrial Accidents Where Poor Shift Handover Was A Contributory FactorDocument2 pages10 Industrial Accidents Where Poor Shift Handover Was A Contributory FactorsgraureNo ratings yet
- Quality Management HandbookDocument8 pagesQuality Management HandbookRambabu komati - QA100% (2)
- SCAT Systematic Cause Analysis TechniqueDocument36 pagesSCAT Systematic Cause Analysis TechniqueWang Fermi100% (1)
- Ykk Training PPT On LocomotiveDocument17 pagesYkk Training PPT On LocomotiverajendraNo ratings yet
- FIELD GUIDE Preventing Serious Injury & FatalitiesGO1965Document16 pagesFIELD GUIDE Preventing Serious Injury & FatalitiesGO1965ekoimampNo ratings yet
- Fmea PDFDocument36 pagesFmea PDFalsoraya00100% (1)
- On The Rig Drilling SystemsDocument10 pagesOn The Rig Drilling Systemscippolippo123No ratings yet
- Types of Human ErrorDocument2 pagesTypes of Human ErrorPankaj PaulNo ratings yet
- CMMSDocument9 pagesCMMSHanna Rizanti KartinaNo ratings yet
- HSSE Pack - Site Training PackDocument36 pagesHSSE Pack - Site Training Packfarhan Ali100% (1)
- 2010 Team Alaska ASH Text Final 10-14-09 ProofDocument251 pages2010 Team Alaska ASH Text Final 10-14-09 ProofjavilapiedraNo ratings yet
- IOGP LSR IntroductionDocument28 pagesIOGP LSR IntroductionharyosetyoNo ratings yet
- Drilling Process Safety 101Document10 pagesDrilling Process Safety 101Saad GhouriNo ratings yet
- Scat EmptyDocument2 pagesScat Emptybuzank buzankNo ratings yet
- Guidelines For Hse AuditingDocument15 pagesGuidelines For Hse AuditingSteppesonNo ratings yet
- RCI Root Cause InvestigationDocument24 pagesRCI Root Cause InvestigationCarlos Jose Sibaja CardozoNo ratings yet
- Inherent Safety Design PrinciplesDocument19 pagesInherent Safety Design PrinciplesAbdurrahman OsailanNo ratings yet
- Safety in Oil and Gas 2015: Driving Improvement in HSE and Process SafetyDocument6 pagesSafety in Oil and Gas 2015: Driving Improvement in HSE and Process SafetyHarthwell CapistranoNo ratings yet
- Pulse - BBS TrainingDocument41 pagesPulse - BBS TrainingRiccardo GastaldoNo ratings yet
- Risk A@ TemplateDocument7 pagesRisk A@ TemplateAlfred LiNo ratings yet
- Human Factor and Reliability Analysis to Prevent Losses in Industrial Processes: An Operational Culture PerspectiveFrom EverandHuman Factor and Reliability Analysis to Prevent Losses in Industrial Processes: An Operational Culture PerspectiveNo ratings yet
- Case Study of British Petroleum and The Deepwater Horizon Disaster of 2010Document6 pagesCase Study of British Petroleum and The Deepwater Horizon Disaster of 2010Abdul Muhaymin MahdiNo ratings yet
- 23.UNIT 5 BP Deepwater Horizon ArraignmentsDocument2 pages23.UNIT 5 BP Deepwater Horizon ArraignmentsRicardoNo ratings yet
- Texas City Refinery Explosion ReportDocument10 pagesTexas City Refinery Explosion ReportNimra JalilNo ratings yet
- Governance Case Study UpdatedDocument7 pagesGovernance Case Study UpdatedJasmine Nouvel Soriaga CruzNo ratings yet
- Glenn Erwin Written StatementDocument4 pagesGlenn Erwin Written StatementNational Commission on the BP Deepwater Horizon Oil Spill and Offshore DrillingNo ratings yet
- Oil Well Cementing Report-NigeriaDocument11 pagesOil Well Cementing Report-Nigerianissefar007No ratings yet
- Method selection study of future P&A at Gjøa fieldDocument136 pagesMethod selection study of future P&A at Gjøa fieldnissefar007No ratings yet
- Creep PDFDocument3 pagesCreep PDFTejas SawantNo ratings yet
- EMW CalculationsDocument3 pagesEMW CalculationsANo ratings yet
- Improving Confidence in Cement Evaluation: Pablo EstradaDocument17 pagesImproving Confidence in Cement Evaluation: Pablo EstradaHassaanAhmed100% (1)
- OGJ - Eight Steps Ensure Successful Cement JobsDocument24 pagesOGJ - Eight Steps Ensure Successful Cement Jobsnissefar007100% (3)
- OGJ - Test Improves Measurement of Cement Slurry StabilityDocument10 pagesOGJ - Test Improves Measurement of Cement Slurry Stabilitynissefar007No ratings yet
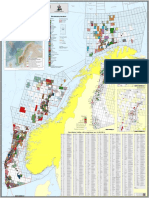
- Map of Norwegian FieldsDocument1 pageMap of Norwegian Fieldsnissefar007No ratings yet
- Oil and Gas CementingDocument15 pagesOil and Gas Cementingnissefar007No ratings yet
- CementingDocument2 pagesCementingnissefar007No ratings yet
- BSSE Presentation To IsraelDocument40 pagesBSSE Presentation To IsraelBrian DunaganNo ratings yet
- Definde CemenvtDocument2 pagesDefinde Cemenvtvindictive666No ratings yet
- Rig Cost - TuDocument1 pageRig Cost - Tunissefar007No ratings yet
- Regulations Relating To Conducting Petroleum Activities (The Activities Regulations)Document25 pagesRegulations Relating To Conducting Petroleum Activities (The Activities Regulations)nissefar007No ratings yet
- V1i4 HPHT Cementing Considerations-Corrected - May 13Document24 pagesV1i4 HPHT Cementing Considerations-Corrected - May 13nissefar007100% (2)
- Hseq4 PrintDocument2 pagesHseq4 Printnissefar007No ratings yet
- Supplementary Paper SP 2 4 HydratesDocument25 pagesSupplementary Paper SP 2 4 Hydrates1234abcdNo ratings yet
- Standards and Guidelines For Drilling, Well Construction and Well Operations - OGP - No485Document2 pagesStandards and Guidelines For Drilling, Well Construction and Well Operations - OGP - No485nissefar007No ratings yet
- Rig Sourcing. Make That Our Job and We'll DeliverDocument1 pageRig Sourcing. Make That Our Job and We'll Delivernissefar007No ratings yet
- Agr Enviro ServiceDocument1 pageAgr Enviro Servicenissefar007No ratings yet
- What Kind of Animal Are YouDocument33 pagesWhat Kind of Animal Are Younissefar007No ratings yet
- A Guide To Well ConstructionDocument127 pagesA Guide To Well ConstructionbimalbkNo ratings yet
- H Drill Chap 4 Dir DrillDocument61 pagesH Drill Chap 4 Dir DrillfabrizioNo ratings yet
- Orda SMDocument2 pagesOrda SMnissefar007No ratings yet
- Shale Gas Extraction in The UK June 2012Document76 pagesShale Gas Extraction in The UK June 2012nissefar007No ratings yet
- Drill String DesignDocument30 pagesDrill String DesignVictor ReyesNo ratings yet
- Casing Design Lesson for Drilling Engineering CourseDocument65 pagesCasing Design Lesson for Drilling Engineering Coursenissefar00750% (2)
- Load History and Buckling of The Production Casing in A HPHT Geothermal WellDocument9 pagesLoad History and Buckling of The Production Casing in A HPHT Geothermal Wellnissefar007No ratings yet
- Halliburton PESA 2010 Spring JanniseDocument29 pagesHalliburton PESA 2010 Spring JanniseFerdana EldriansyahNo ratings yet
- Fluid Mosaic Paper PDFDocument0 pagesFluid Mosaic Paper PDFDina Kharida100% (1)
- Handout TMA GuidanceDocument3 pagesHandout TMA GuidanceElizabeth FernandezNo ratings yet
- ManualDocument572 pagesManualjoejunkisNo ratings yet
- Landscapes of Emotion 1991Document346 pagesLandscapes of Emotion 1991Rachmad AdilaNo ratings yet
- The Sensitivity of The Bielschowsky Head-Tilt Test in Diagnosing Acquired Bilateral Superior Oblique ParesisDocument10 pagesThe Sensitivity of The Bielschowsky Head-Tilt Test in Diagnosing Acquired Bilateral Superior Oblique ParesisAnonymous mvNUtwidNo ratings yet
- The Impact of Training and Development On Employee Perfornace: A Case Study On Meena BazarDocument8 pagesThe Impact of Training and Development On Employee Perfornace: A Case Study On Meena BazarAcademia PapersNo ratings yet
- SLR140 - ArDocument51 pagesSLR140 - ArDeepak Ojha100% (1)
- ISO - 8041.2005 - Human - Response - To - Vibrations - Measuring - Instrumentation PDFDocument98 pagesISO - 8041.2005 - Human - Response - To - Vibrations - Measuring - Instrumentation PDFraffacapNo ratings yet
- Topics For Grade 7 ScienceDocument200 pagesTopics For Grade 7 ScienceShaynie Mhe Amar Antonio67% (3)
- Understanding A Brain Based Approach To Learning PDFDocument6 pagesUnderstanding A Brain Based Approach To Learning PDFChandrika SimadereyNo ratings yet
- Measurement Circularity Preview - GDTDocument8 pagesMeasurement Circularity Preview - GDTllmm_088No ratings yet
- Battlestars VsDocument56 pagesBattlestars VsSkiman94100% (2)
- Practical Research 1 ExamDocument4 pagesPractical Research 1 ExamAlvin Montes100% (1)
- Cover Page ( (DLW 5013) ) 11 April 2020 - .222 PDFDocument4 pagesCover Page ( (DLW 5013) ) 11 April 2020 - .222 PDFElamaaran AlaggarNo ratings yet
- Quantiacs Reading ListDocument7 pagesQuantiacs Reading Listdesikudi9000No ratings yet
- JPIA Manual Membership SystemDocument50 pagesJPIA Manual Membership SystemEdita Lamp DizonNo ratings yet
- Notification JNTU Anantapur Assistant Professor Posts PDFDocument7 pagesNotification JNTU Anantapur Assistant Professor Posts PDFNagabhushanaNo ratings yet
- The Real Case For Aushwitz - Carlo Mattogno PDFDocument692 pagesThe Real Case For Aushwitz - Carlo Mattogno PDFJordan100% (3)
- Course DeconDocument6 pagesCourse DeconSilvia Jannatul FajarNo ratings yet
- Lab 4.5.1 Observing TCP and UDP Using Netstat (Instructor Version)Document7 pagesLab 4.5.1 Observing TCP and UDP Using Netstat (Instructor Version)Rifqi Imaduddin IrfanNo ratings yet
- Dramatic Nuclear Winter Concept Art WorkshopDocument5 pagesDramatic Nuclear Winter Concept Art WorkshopArc AngleNo ratings yet
- F8 Chapter 01Document3 pagesF8 Chapter 01Tay Joo FangNo ratings yet
- Panasonic - PDP TH 37 42 pv70xx - Gph10deDocument85 pagesPanasonic - PDP TH 37 42 pv70xx - Gph10defaroltek0% (1)
- Summarizing and ParaphrasingDocument2 pagesSummarizing and ParaphrasingKylle VillafloresNo ratings yet
- Millipore AcademicDocument93 pagesMillipore Academickron541No ratings yet
- G10 Q3 PPT3Document20 pagesG10 Q3 PPT3Ma. Shiela Mira NarceNo ratings yet
- Principles of Management All ChaptersDocument263 pagesPrinciples of Management All ChaptersRushabh Vora81% (21)
- THEORY Transformation Question BankDocument7 pagesTHEORY Transformation Question Bankpankaj12345katreNo ratings yet
- The Freemason S Monitor-Thomas Smith WebbDocument335 pagesThe Freemason S Monitor-Thomas Smith WebbJORGE LUIZ DE A LINSNo ratings yet
- Apsa StyleDocument4 pagesApsa StyleLincoln DerNo ratings yet