You might also like
- 2e Volume1 2016 PDFDocument1,361 pages2e Volume1 2016 PDFNenny Puji LestariNo ratings yet
- 4 High Alert Medication FinalDocument4 pages4 High Alert Medication Finalrini setyawatiNo ratings yet
- Gabungan Presentasi StrategizingDocument45 pagesGabungan Presentasi StrategizingNenny Puji LestariNo ratings yet
- DHF Menurut WHO 2011Document212 pagesDHF Menurut WHO 2011Jamal SutrisnaNo ratings yet
- 2e Volume1 2016 PDFDocument1,361 pages2e Volume1 2016 PDFNenny Puji LestariNo ratings yet
- Patient Safety USMLEDocument18 pagesPatient Safety USMLEsdroyafmc100% (2)
- Applying Health Education Theory To Patient Safety PDFDocument8 pagesApplying Health Education Theory To Patient Safety PDFNenny Puji LestariNo ratings yet
- DHF Menurut WHO 2011Document212 pagesDHF Menurut WHO 2011Jamal SutrisnaNo ratings yet
- Investigating Organizational Quality Improvement PDFDocument11 pagesInvestigating Organizational Quality Improvement PDFNenny Puji LestariNo ratings yet
- V3 Eng PDFDocument848 pagesV3 Eng PDFaidhaNo ratings yet
- 035 HQ Vol13 No1 Heenan PDFDocument8 pages035 HQ Vol13 No1 Heenan PDFNenny Puji LestariNo ratings yet
- Development Report For PS PDFDocument4 pagesDevelopment Report For PS PDFNenny Puji LestariNo ratings yet
- Impact of Quality Strategies On Hospital Outputs PDFDocument8 pagesImpact of Quality Strategies On Hospital Outputs PDFNenny Puji LestariNo ratings yet
- ImprovingCommunicationPART2 PDFDocument23 pagesImprovingCommunicationPART2 PDFNenny Puji LestariNo ratings yet
- Health Seeking BehaviorDocument37 pagesHealth Seeking BehaviorAristya Ekaputra100% (1)
- Initiative To Implement 6 Key Measures PDFDocument2 pagesInitiative To Implement 6 Key Measures PDFNenny Puji LestariNo ratings yet
- Medicsafety Qual 2009 PDFDocument10 pagesMedicsafety Qual 2009 PDFNenny Puji LestariNo ratings yet
- Proactive Approaches To Safety Management Thought Paper PDFDocument11 pagesProactive Approaches To Safety Management Thought Paper PDFNenny Puji LestariNo ratings yet
- Making Patient Safety The Centerpiece PDFDocument4 pagesMaking Patient Safety The Centerpiece PDFNenny Puji LestariNo ratings yet
- Education PDFDocument6 pagesEducation PDFNenny Puji LestariNo ratings yet
- Critical Incidence Reporting & Learning PDFDocument7 pagesCritical Incidence Reporting & Learning PDFNenny Puji LestariNo ratings yet
- Assesing P Safety PDFDocument10 pagesAssesing P Safety PDFNenny Puji LestariNo ratings yet
- Central or Local Incident Reporting PDFDocument5 pagesCentral or Local Incident Reporting PDFNenny Puji LestariNo ratings yet
- Advances Adams Pizarro - 109 PDFDocument20 pagesAdvances Adams Pizarro - 109 PDFNenny Puji LestariNo ratings yet
- Who Will Care For Us PDFDocument44 pagesWho Will Care For Us PDFNenny Puji LestariNo ratings yet
- Advances-Meyer 41 PDFDocument13 pagesAdvances-Meyer 41 PDFNenny Puji LestariNo ratings yet
- Time To Accelerate Integration of Human Factors and Ergonomics in Patient Safety PDFDocument5 pagesTime To Accelerate Integration of Human Factors and Ergonomics in Patient Safety PDFNenny Puji LestariNo ratings yet
- The Disclosure Dilemma - Large-Scale Adverse Events PDFDocument9 pagesThe Disclosure Dilemma - Large-Scale Adverse Events PDFNenny Puji LestariNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Strategies For Dengue Control ProgramDocument22 pagesStrategies For Dengue Control ProgramNaseem QaziNo ratings yet
- Cognitive Behavioral Therapy For Managing PainDocument3 pagesCognitive Behavioral Therapy For Managing PainJustus K GatheruNo ratings yet
- Vii. NCP and Case Study: Learn The DemonstrateDocument4 pagesVii. NCP and Case Study: Learn The DemonstrateVenus Glaze Verzola100% (2)
- Social Worker MSWDocument2 pagesSocial Worker MSWapi-1213661170% (1)
- Chronic Renal FailureDocument13 pagesChronic Renal FailureAnusha VergheseNo ratings yet
- Community Health Bag Nursing ProceduresDocument10 pagesCommunity Health Bag Nursing Proceduresmariet abraham100% (1)
- Biology ProjectDocument18 pagesBiology ProjectParamdeep Singh100% (1)
- Factors Influencing Provision of Basic Emergency Obstetric Care Services in Luzon, PhilippinesDocument12 pagesFactors Influencing Provision of Basic Emergency Obstetric Care Services in Luzon, PhilippinesIJPHSNo ratings yet
- A Case Study On Tamaka Swasa W. S. R To Bronchial Asthma AyurvedaDocument2 pagesA Case Study On Tamaka Swasa W. S. R To Bronchial Asthma AyurvedaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 09 18 06 Module On Obstetric PathologyDocument30 pages09 18 06 Module On Obstetric Pathology2012No ratings yet
- Emergency Nursing & Critical CareDocument74 pagesEmergency Nursing & Critical Carenursereview100% (14)
- Annals of International Medical and Dental ResearchDocument4 pagesAnnals of International Medical and Dental ResearchDr Rohit varshneyNo ratings yet
- NCP EmphysemaDocument9 pagesNCP Emphysemahermesdave188% (8)
- Transmission Precautions ExplainedDocument8 pagesTransmission Precautions Explainedniraj_sd100% (1)
- Tumor Necrosis Factor Inhibitors in Patients With Takayasu Arteritis: Experience From A Referral Center With Long-Term FollowupDocument5 pagesTumor Necrosis Factor Inhibitors in Patients With Takayasu Arteritis: Experience From A Referral Center With Long-Term FollowupMikhail PisarevNo ratings yet
- Chapter Quiz for Antimicrobial AgentsDocument1 pageChapter Quiz for Antimicrobial AgentsIrwan M. IskoberNo ratings yet
- Legal MEd - QuizDocument1 pageLegal MEd - Quizcbac1990No ratings yet
- Inclusion Body Hepatitis Hydropericarditis Litchi Heart Syndrome in Broiler ChickenDocument39 pagesInclusion Body Hepatitis Hydropericarditis Litchi Heart Syndrome in Broiler ChickenDr.Kedar Karki ,M.V.Sc.Preventive Vet.Medicine CLSU PhilippinesNo ratings yet
- June 2014 Questions Returned From Candidates - Thank You: Long Case 1Document14 pagesJune 2014 Questions Returned From Candidates - Thank You: Long Case 1karan270No ratings yet
- K & E CH 33 HygieneDocument98 pagesK & E CH 33 HygieneJacqueline Greer100% (2)
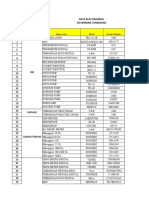
- Data Alat Kalibrasi Rs TNGDocument10 pagesData Alat Kalibrasi Rs TNGHelena LowaNo ratings yet
- General Medicine Proficiency CertificateDocument179 pagesGeneral Medicine Proficiency CertificateManoj Kumar GuptaNo ratings yet
- Asthma Case Scenario: Symptoms, Risk Factors, Examination, Investigations and ManagementDocument10 pagesAsthma Case Scenario: Symptoms, Risk Factors, Examination, Investigations and ManagementFemale calmNo ratings yet
- Sample CollectionDocument18 pagesSample Collectioncawsey mohamedNo ratings yet
- Life-members-Indian Medico-Legal & Ethics Association (Imlea) - Mix State & Mix DepartmentDocument64 pagesLife-members-Indian Medico-Legal & Ethics Association (Imlea) - Mix State & Mix DepartmentKriti Kumari100% (1)
- Ic Healthcare Plan Guide Eng 0420 PDFDocument28 pagesIc Healthcare Plan Guide Eng 0420 PDFrobinmathew77No ratings yet
- Breakthroughs That Change Patients' Lives: Annual ReviewDocument56 pagesBreakthroughs That Change Patients' Lives: Annual ReviewAnindita SahaNo ratings yet
- KINDER 1 (AutoRecovered)Document3 pagesKINDER 1 (AutoRecovered)rhodNo ratings yet
- Funda Set 2Document36 pagesFunda Set 2Dick Morgan FerrerNo ratings yet
- StarHealthAssureInsurancePolicy BrochureDocument13 pagesStarHealthAssureInsurancePolicy Brochurepradosh002No ratings yet