You might also like
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Highland Guidelines - LDK 2013-2-15Document3 pagesHighland Guidelines - LDK 2013-2-15andrew herringNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Rib Fracture SerratusDocument3 pagesRib Fracture Serratusandrew herring100% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Roux 2013Document7 pagesRoux 2013andrew herringNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Buprenorphine 2016-7-18Document1 pageBuprenorphine 2016-7-18andrew herringNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- K Opiods For Pain BupDocument2 pagesK Opiods For Pain Bupandrew herringNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Herring ED Intractable Abdominal pain-N+VDocument1 pageHerring ED Intractable Abdominal pain-N+Vandrew herringNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Intravenous Lidocaine To Treat Postoperative Pain : Lidocaína Intravenosa No Tratamento Da Dor Pós-OperatóriaDocument6 pagesIntravenous Lidocaine To Treat Postoperative Pain : Lidocaína Intravenosa No Tratamento Da Dor Pós-Operatóriaandrew herringNo ratings yet
- Original Article: Serratus Plane Block: A Novel Ultrasound-Guided Thoracic Wall Nerve BlockDocument7 pagesOriginal Article: Serratus Plane Block: A Novel Ultrasound-Guided Thoracic Wall Nerve Blockandrew herringNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Rib Fracture W: PecsDocument8 pagesRib Fracture W: Pecsandrew herring100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- 3.2.16.highland Emergency Medicine Journal Club Methods.2Document2 pages3.2.16.highland Emergency Medicine Journal Club Methods.2andrew herringNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Ultrasound-Guided Block of TheDocument6 pagesUltrasound-Guided Block of Theandrew herringNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Ketamine As Rescue Treatment FDocument8 pagesKetamine As Rescue Treatment Fandrew herringNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Dex For Dental Pain & SwellingDocument7 pagesDex For Dental Pain & Swellingandrew herring100% (1)
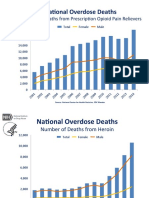
- OPR - Heroin DeathsDocument2 pagesOPR - Heroin Deathsandrew herringNo ratings yet
- Nej MR A 1511480Document9 pagesNej MR A 1511480Tohari Masidi AminNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- CVS Action Plan v2Document1 pageCVS Action Plan v2andrew herringNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Ultrasound Guided Interventional Procedures In.13Document14 pagesUltrasound Guided Interventional Procedures In.13andrew herring100% (1)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Ultrasound Guided Interventional Procedures In.4Document13 pagesUltrasound Guided Interventional Procedures In.4andrew herringNo ratings yet
- APA Unknown Lab ReportDocument9 pagesAPA Unknown Lab ReportMiss DNo ratings yet
- SHC Heme Onc Antimicrobial ProphylaxisDocument4 pagesSHC Heme Onc Antimicrobial ProphylaxisTala MahmoudNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Diabetes Mellitus Surgical PatientDocument33 pagesDiabetes Mellitus Surgical PatientGerald AndersonNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Abstract Cagilkayan New1Document2 pagesAbstract Cagilkayan New1cagilkayanNo ratings yet
- Chlamydia Power PointDocument19 pagesChlamydia Power PointAnne McfarlandNo ratings yet
- Material 3 - Acute Kidney Injury in Children - Fauziah Rudhiati, MKep., Sp. Kep - An PDFDocument21 pagesMaterial 3 - Acute Kidney Injury in Children - Fauziah Rudhiati, MKep., Sp. Kep - An PDFINTAN MADULARANo ratings yet
- Anemia - AMBOSSDocument2 pagesAnemia - AMBOSStgayuNo ratings yet
- Nemeroff Et Al. 2013 - Dsm-5 2013 Collection Psychiatrist Views (Word Drop)Document19 pagesNemeroff Et Al. 2013 - Dsm-5 2013 Collection Psychiatrist Views (Word Drop)DestriNo ratings yet
- Atlas of The Global Egg IndustryDocument36 pagesAtlas of The Global Egg IndustryJNo ratings yet
- Bariatric Surgery PresentationDocument25 pagesBariatric Surgery PresentationAHMEDNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Hypomagnesemic Tetany in Calve1Document1 pageHypomagnesemic Tetany in Calve1Morad ImadNo ratings yet
- Indian Star TortiseDocument189 pagesIndian Star TortiseManish HunkNo ratings yet
- Fiitjee: Talent Reward Exam - 2020Document25 pagesFiitjee: Talent Reward Exam - 2020Imtesalur Rahman100% (1)
- CPE239 Demonstration 411Document11 pagesCPE239 Demonstration 411Hong Jun TeeNo ratings yet
- Adrenergic and Cholinergic SummaryDocument2 pagesAdrenergic and Cholinergic Summaryhashman0689No ratings yet
- B PharmDocument69 pagesB PharmShubham BansalNo ratings yet
- Articular Disc Displacement Disorders and Its Prosthodontic Management: A Literature ReviewDocument9 pagesArticular Disc Displacement Disorders and Its Prosthodontic Management: A Literature ReviewTopan MuhamadNo ratings yet
- 06 Msds Ripoxy R-802 ExDocument9 pages06 Msds Ripoxy R-802 ExAnto Maryadi100% (1)
- Strategic Group Minutes October 7th 2021 DraftDocument10 pagesStrategic Group Minutes October 7th 2021 Draftapi-349611130No ratings yet
- 1 s2.0 S2095809918301887 MainDocument15 pages1 s2.0 S2095809918301887 MainBudi Utami FahnunNo ratings yet
- AbtrascDocument2 pagesAbtrascbebo94No ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- McKay Hard Facing Electrodes MsdsDocument2 pagesMcKay Hard Facing Electrodes MsdssalcabesNo ratings yet
- (Cambridge Medicine) Ian Calder - Adrian C Pearce-Core Topics in Airway Management-Cambridge University Press (2011) PDFDocument330 pages(Cambridge Medicine) Ian Calder - Adrian C Pearce-Core Topics in Airway Management-Cambridge University Press (2011) PDFM Victoria SalazarNo ratings yet
- 308 Case 25.05.20Document17 pages308 Case 25.05.20DeshGujarat80% (5)
- Knolegde On The Cause and Prevention of Anemai in Prganant Women at The Buea Regional HospitalDocument30 pagesKnolegde On The Cause and Prevention of Anemai in Prganant Women at The Buea Regional HospitalGwagsiGlennNo ratings yet
- CH 11 The Extracellular Matrix and Cell InteractionsDocument24 pagesCH 11 The Extracellular Matrix and Cell InteractionsCyrene John CruzNo ratings yet
- Ent RevisionDocument104 pagesEnt RevisionNano BaddourNo ratings yet
- Hospital Practice & Patient CareDocument14 pagesHospital Practice & Patient CareAkinsola Ayomidotun100% (1)
- Subgingival Microbial Changes During The First 3 Months of Fixed Appliance Treatment in Female Adult PatientsDocument9 pagesSubgingival Microbial Changes During The First 3 Months of Fixed Appliance Treatment in Female Adult PatientsAprilia FajrinNo ratings yet
- Medical Terminology Express A Short Course Approach by Body System 2nd Edition Gylys Test BankDocument14 pagesMedical Terminology Express A Short Course Approach by Body System 2nd Edition Gylys Test BankSaraRogersrbwgd100% (18)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- Bitten: The Secret History of Lyme Disease and Biological WeaponsFrom EverandBitten: The Secret History of Lyme Disease and Biological WeaponsRating: 3.5 out of 5 stars3.5/5 (11)
- Do You Believe in Magic?: The Sense and Nonsense of Alternative MedicineFrom EverandDo You Believe in Magic?: The Sense and Nonsense of Alternative MedicineNo ratings yet