You might also like
- Artikel TherapyDocument6 pagesArtikel TherapyKyra ModestyNo ratings yet
- Jurnal DR Nawan 1Document7 pagesJurnal DR Nawan 1muntiir gurusingaNo ratings yet
- 13-10 Topic 7. Complicated PneumoniaDocument35 pages13-10 Topic 7. Complicated PneumoniaReza Ervanda ZilmiNo ratings yet
- Treatment of Acute Viral Bronchiolitis: Ernst EberDocument6 pagesTreatment of Acute Viral Bronchiolitis: Ernst EberDyah Gaby KesumaNo ratings yet
- Proposal To Include Antibacterial Drugs For Treating Upper and Lower Respiratory Infections in ChildrenDocument52 pagesProposal To Include Antibacterial Drugs For Treating Upper and Lower Respiratory Infections in ChildrenAznil FajriNo ratings yet
- 1.e. Bronchiolitis Treatment & Management - Approach Considerations, Initial Management, Admission CriteriaDocument12 pages1.e. Bronchiolitis Treatment & Management - Approach Considerations, Initial Management, Admission CriteriaDavid CraigNo ratings yet
- Quality of Nurs-WPS OfficeDocument2 pagesQuality of Nurs-WPS OfficeLjc JaslinNo ratings yet
- Bronchiolitis in Infants and Children - Treatment, Outcome, and Prevention - UpToDateDocument35 pagesBronchiolitis in Infants and Children - Treatment, Outcome, and Prevention - UpToDatenathalia_pastasNo ratings yet
- Community-Acquired Bacterial Pneumonia in Children....Document6 pagesCommunity-Acquired Bacterial Pneumonia in Children....MariaNo ratings yet
- Bronchiolitis in Infants and Children - Treatment, Outcome, and Prevention - UpToDateDocument25 pagesBronchiolitis in Infants and Children - Treatment, Outcome, and Prevention - UpToDateAlejandra AubadNo ratings yet
- Bronquiolitis TXDocument36 pagesBronquiolitis TXDauris garcia diazNo ratings yet
- Who/Unicef Joint StatementDocument8 pagesWho/Unicef Joint Statementyuni020670No ratings yet
- Summary (Pedia)Document1 pageSummary (Pedia)JA BerzabalNo ratings yet
- PediaDocument2 pagesPediaCharlaine Gripal SudlaNo ratings yet
- CAP Guidelines SA 2020Document22 pagesCAP Guidelines SA 2020kudzaimuregidubeNo ratings yet
- Thorax 2008 Shields Iii1 Iii15Document16 pagesThorax 2008 Shields Iii1 Iii15diapalupiNo ratings yet
- Acute Cough (Bronchitis) : 2011 UpdateDocument4 pagesAcute Cough (Bronchitis) : 2011 UpdatecorsaruNo ratings yet
- IDSA Clinical Practice Guideline For Acute Bacterial Rhino Sinusitis in Children and AdultsDocument41 pagesIDSA Clinical Practice Guideline For Acute Bacterial Rhino Sinusitis in Children and AdultsKarina ParedesNo ratings yet
- Articulos BronquiolitisDocument18 pagesArticulos BronquiolitisLaura López Del Castillo LalydelcaNo ratings yet
- Bronquiolitis IIDocument48 pagesBronquiolitis IIISABELA GUEVARA ESPAÑANo ratings yet
- Management and Treatment Guidelines For Sepsis in Pediatric PatientsDocument9 pagesManagement and Treatment Guidelines For Sepsis in Pediatric PatientsIhsan PutraNo ratings yet
- Prophylactics of PneumoniaDocument31 pagesProphylactics of PneumoniaJoisy AloorNo ratings yet
- CPG Management of Childhood Asthma (2014)Document20 pagesCPG Management of Childhood Asthma (2014)Haz100% (1)
- Pediatric PneumoniaDocument12 pagesPediatric PneumoniaKrystal Migo Denolo ContrerasNo ratings yet
- Cystic Fibrosis Advances in The Management of Cystic FibrosisDocument19 pagesCystic Fibrosis Advances in The Management of Cystic FibrosisMehtab AlamNo ratings yet
- HK-guide CAP in ChildrenDocument17 pagesHK-guide CAP in ChildrenXi JIANo ratings yet
- Treatment of Recurrent Virus-Induced Wheezing in Young Children - UpToDateDocument27 pagesTreatment of Recurrent Virus-Induced Wheezing in Young Children - UpToDateandreza.beatrizNo ratings yet
- Accepted Manuscript: Paediatric Respiratory ReviewsDocument32 pagesAccepted Manuscript: Paediatric Respiratory ReviewslaurentiaNo ratings yet
- PHD Thesis Samuel Coenen PDFDocument172 pagesPHD Thesis Samuel Coenen PDFsamuel_coenenNo ratings yet
- 01 ProjectDocument30 pages01 Projectkarunyabathula100% (1)
- The Challenge of Tuberculosis in Developing Countries: International Journal of Infection ControlDocument2 pagesThe Challenge of Tuberculosis in Developing Countries: International Journal of Infection Controlaulia_khairani_1No ratings yet
- Bronchiolitis: Juan Manuel LozanoDocument18 pagesBronchiolitis: Juan Manuel LozanoFelipe CamposNo ratings yet
- Management of COPD in Primary and Secondary Care, TheFrom EverandManagement of COPD in Primary and Secondary Care, TheRating: 5 out of 5 stars5/5 (1)
- Diagnosis and Treatment of Chronic CoughFrom EverandDiagnosis and Treatment of Chronic CoughSang Heon ChoNo ratings yet
- Rhinopharyngeal Retrograde Clearance Induces Less Respiratory Effort and Fewer Adverse Effects in Comparison With Nasopharyngeal Aspiration in Infants With Acute Viral BronchiolitisDocument7 pagesRhinopharyngeal Retrograde Clearance Induces Less Respiratory Effort and Fewer Adverse Effects in Comparison With Nasopharyngeal Aspiration in Infants With Acute Viral Bronchiolitismariane bezerraNo ratings yet
- Edit NG Drug StudyDocument35 pagesEdit NG Drug StudyAlleinad BarracasNo ratings yet
- Acute Sinusitis and Sore Throat in Primary Care: Chris Del MarDocument3 pagesAcute Sinusitis and Sore Throat in Primary Care: Chris Del MarRhahima SyafrilNo ratings yet
- PCAP UpdatesDocument60 pagesPCAP UpdatesMarko ParungoNo ratings yet
- E013796 FullDocument13 pagesE013796 FullRenny HusnulNo ratings yet
- Pediatric Ward Journal Binwag BSN 2aDocument2 pagesPediatric Ward Journal Binwag BSN 2aVincentus BinNo ratings yet
- BronchopneumoniaDocument13 pagesBronchopneumoniaSabella Gustika VernandaNo ratings yet
- Essential Update: Pediatric Pneumonia May Be Effectively Treated With Twice-Daily AmoxicillinDocument54 pagesEssential Update: Pediatric Pneumonia May Be Effectively Treated With Twice-Daily AmoxicillinYostesara Maurena SantosaNo ratings yet
- Keeping Asthma at BayDocument9 pagesKeeping Asthma at BayLorenn AdarnaNo ratings yet
- 10 1164@rccm 201910-1934CI PDFDocument23 pages10 1164@rccm 201910-1934CI PDFMuhammad Arief SaputraNo ratings yet
- A Case Report On Management of Severe Childhood Pneumonia in Low Resource SettingsDocument5 pagesA Case Report On Management of Severe Childhood Pneumonia in Low Resource SettingsUparsariya Pratik Sureshbhai (Student BSMU. Chernivtsi)No ratings yet
- Jurnal BronkiolitisDocument10 pagesJurnal BronkiolitisAmi WilliamsNo ratings yet
- Special Issue ARTICLE Less Is More: Evidence-Based Management of BronchiolitisDocument11 pagesSpecial Issue ARTICLE Less Is More: Evidence-Based Management of BronchiolitisyundaNo ratings yet
- Cost-Utility Analysis of A Pharmacy-Led Self-Management Programme For Patients With COPDDocument10 pagesCost-Utility Analysis of A Pharmacy-Led Self-Management Programme For Patients With COPDoktarina puspitasariNo ratings yet
- A Randomised Dose-Ranging Study of Tiotropium Respimat® in Children With Symptomatic Asthma Despite Inhaled CorticosteroidsDocument10 pagesA Randomised Dose-Ranging Study of Tiotropium Respimat® in Children With Symptomatic Asthma Despite Inhaled CorticosteroidsabdmaliknasNo ratings yet
- Hamza DissertDocument108 pagesHamza DissertMobin Ur Rehman KhanNo ratings yet
- Tuberculosis Thesis TitleDocument5 pagesTuberculosis Thesis Titletjgyhvjef100% (2)
- MDRTB Case StudyDocument35 pagesMDRTB Case StudyFejlean Angelica AntineoNo ratings yet
- Community-Acquired Pneumonia in Children - Outpatient Treatment - UpToDateDocument38 pagesCommunity-Acquired Pneumonia in Children - Outpatient Treatment - UpToDateJosué Pablo Chicaiza AbadNo ratings yet
- Judicious Use of Antibiotics: A Guide For Oregon CliniciansDocument32 pagesJudicious Use of Antibiotics: A Guide For Oregon CliniciansRiyan SaputraNo ratings yet
- NCM 121 Evidence-Based JournalDocument4 pagesNCM 121 Evidence-Based JournalAngela PareNo ratings yet
- Treat Pneumonia With The Wonder DrugsDocument3 pagesTreat Pneumonia With The Wonder DrugsbobbyramakantNo ratings yet
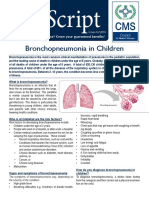
- Bronchopneumonia in ChildrenDocument3 pagesBronchopneumonia in ChildrenputraNo ratings yet
- Therapy For Bronchiolitis: When Some Become None: EditorialsDocument3 pagesTherapy For Bronchiolitis: When Some Become None: Editorialsputrikartikasari91No ratings yet
- Efek Probiotik Pada Bayi Dengan Diare AkutDocument7 pagesEfek Probiotik Pada Bayi Dengan Diare AkutRizal ItemNo ratings yet
- Aspect Tumor Fkk-UmjDocument30 pagesAspect Tumor Fkk-Umjakbarsp1No ratings yet
- Effect of Pnemococcal Conjugate Vaccine On Pnemococcal MeningitisDocument13 pagesEffect of Pnemococcal Conjugate Vaccine On Pnemococcal Meningitisakbarsp1No ratings yet
- Aspiration Pneumonia SPDocument33 pagesAspiration Pneumonia SPakbarsp1No ratings yet
- Alpha ThalassemiaDocument2 pagesAlpha ThalassemiawhcaoNo ratings yet
- The Management of Community Acquired Pneumonia in ChildhoodDocument4 pagesThe Management of Community Acquired Pneumonia in Childhoodakbarsp1No ratings yet
- Phase 1: Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 7Document2 pagesPhase 1: Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 7akbarsp1No ratings yet
- 151 MakalahDocument12 pages151 MakalahMissda MNsNo ratings yet
- Rasionalisasi Obat HerbalDocument33 pagesRasionalisasi Obat Herbalakbarsp1No ratings yet
- DF Birth Weight Body Mass Index and Asma in Youn Adults PDFDocument8 pagesDF Birth Weight Body Mass Index and Asma in Youn Adults PDFakbarsp1No ratings yet
- PadDocument5 pagesPadA Yusril IzzaNo ratings yet
- 7-Hubungan Faktor Risiko Umur Jenis Kelamin Kegemukan-Jelantik HaryatiDocument6 pages7-Hubungan Faktor Risiko Umur Jenis Kelamin Kegemukan-Jelantik Haryatisiti rahmahNo ratings yet
- Pedoman SurveilansDocument24 pagesPedoman SurveilansLukas83% (18)
- 121 323 1 PB PDFDocument7 pages121 323 1 PB PDFakbarsp1No ratings yet
- 162 Lili Nurmawati G2C206009 A PDFDocument3 pages162 Lili Nurmawati G2C206009 A PDFakbarsp1No ratings yet
- 680 1253 1 SM PDFDocument7 pages680 1253 1 SM PDFakbarsp1No ratings yet
- The Lucid Dream Exchange Magazine Issue 36Document36 pagesThe Lucid Dream Exchange Magazine Issue 36api-384230967% (3)
- Marathi Book ListDocument4 pagesMarathi Book ListGajanan PatilNo ratings yet
- Marketing Mix 4P's and SWOT Analysis of OLPERSDocument3 pagesMarketing Mix 4P's and SWOT Analysis of OLPERSSaad AliNo ratings yet
- Travel To Egypt: Conversation Cheat SheetDocument2 pagesTravel To Egypt: Conversation Cheat SheetNasima BegumNo ratings yet
- c238 Service ManualDocument2,304 pagesc238 Service Manualcody100% (1)
- Advanced Space Propulsion Based On VacuumDocument17 pagesAdvanced Space Propulsion Based On VacuumMystery Wire100% (1)
- Samsung Galaxy Beam GT I8530 User ManualDocument172 pagesSamsung Galaxy Beam GT I8530 User ManualFirdaus AhmadNo ratings yet
- Dengue Syndrome: Presented By: A.Sahaya Mary M.SC Nursing I Yr Scon, SimatsDocument57 pagesDengue Syndrome: Presented By: A.Sahaya Mary M.SC Nursing I Yr Scon, Simatssagi muNo ratings yet
- Tesla Roadster (A) 2014Document25 pagesTesla Roadster (A) 2014yamacNo ratings yet
- M.Vikram: Department of Electronics and Communication EngineeringDocument26 pagesM.Vikram: Department of Electronics and Communication EngineeringSyed AmaanNo ratings yet
- Payment System - Basic Schemes: July 2020Document11 pagesPayment System - Basic Schemes: July 2020Amirul Amin IVNo ratings yet
- Coronavirus Disease (COVID-19) : Situation Report - 125Document17 pagesCoronavirus Disease (COVID-19) : Situation Report - 125CityNewsTorontoNo ratings yet
- Ygg 07Document44 pagesYgg 07JemGirlNo ratings yet
- Technipfmc Corporate Brochure en 2018Document7 pagesTechnipfmc Corporate Brochure en 2018Sivaji RajinikanthNo ratings yet
- Success Criteria For Change InitiativesDocument6 pagesSuccess Criteria For Change Initiativesgimmeanearful100% (1)
- Matisse As Printmaker: Matisse'S Printmaking ProcessesDocument2 pagesMatisse As Printmaker: Matisse'S Printmaking ProcessesWriterIncNo ratings yet
- Unemployment InsuranceDocument8 pagesUnemployment InsuranceBhumani TyagiNo ratings yet
- Very Important General Knowledge MCQs With DetailsDocument13 pagesVery Important General Knowledge MCQs With DetailsNiaz AsgharNo ratings yet
- A Muslim Reformist in Communist Yugoslavia The Life and Thought of Husein Äx90 Ozo (Husein Mekic, Sejad) (Z-Library)Document212 pagesA Muslim Reformist in Communist Yugoslavia The Life and Thought of Husein Äx90 Ozo (Husein Mekic, Sejad) (Z-Library)Raeed IslamNo ratings yet
- Janet P. Espada Et Al., Challenges in The Implementation of The Mother Tongue-Based Multilingual Education Program:A Case StudyDocument19 pagesJanet P. Espada Et Al., Challenges in The Implementation of The Mother Tongue-Based Multilingual Education Program:A Case StudyAnalyn Bintoso DabanNo ratings yet
- Telangana Peasants Armed StruggleDocument9 pagesTelangana Peasants Armed StruggleSudheer KolachinaNo ratings yet
- Wheel Loader wl56Document6 pagesWheel Loader wl56Shahzad AliNo ratings yet
- Commonwealth Essay Competition 2014Document2 pagesCommonwealth Essay Competition 2014q998No ratings yet
- Anatomy of A Resume 2Document4 pagesAnatomy of A Resume 2Anna CruzNo ratings yet
- Microsoft Lumia 950 XL - Unlocked (Black)Document8 pagesMicrosoft Lumia 950 XL - Unlocked (Black)Dawood AhmedNo ratings yet
- Rudolf Steiner - The Gospel of ST MarkDocument218 pagesRudolf Steiner - The Gospel of ST Markhumblejoe100% (9)
- C++ & Object Oriented Programming: Dr. Alekha Kumar MishraDocument23 pagesC++ & Object Oriented Programming: Dr. Alekha Kumar MishraPriyanshu Kumar KeshriNo ratings yet
- Environmental Education Strategy (2010-2014) : United Republic of TanzaniaDocument63 pagesEnvironmental Education Strategy (2010-2014) : United Republic of Tanzaniaalli sheeranNo ratings yet
- The Oxford Handbook of The Trinity (Introducción)Document12 pagesThe Oxford Handbook of The Trinity (Introducción)casandraentroya100% (1)
- People vs. Samson, September 2, 2015Document5 pagesPeople vs. Samson, September 2, 2015Alpha Grace JugalNo ratings yet