You might also like
- Handbook of Current and Novel Protocols for the Treatment of InfertilityFrom EverandHandbook of Current and Novel Protocols for the Treatment of InfertilityMichael H. DahanNo ratings yet
- 2023 OB/GYN Coding Manual: Components of Correct CodingFrom Everand2023 OB/GYN Coding Manual: Components of Correct CodingNo ratings yet
- Anesthesia For Hysteroscopy: A Comparison of General and Spinal AnesthesiaDocument7 pagesAnesthesia For Hysteroscopy: A Comparison of General and Spinal AnesthesiaIJAR JOURNALNo ratings yet
- Obstetrics, Gynaecology-Textbook of Obstetrics and Gynaecology For Medical Students, 2nd Edition-Akin Agboola-2006Document559 pagesObstetrics, Gynaecology-Textbook of Obstetrics and Gynaecology For Medical Students, 2nd Edition-Akin Agboola-2006fagiy51113No ratings yet
- Dystocia and Augmentation of LAbor PDFDocument10 pagesDystocia and Augmentation of LAbor PDFKathleenNo ratings yet
- Laparoscopic Gynecologist Surgeon in HSR Layout BangaloreDocument8 pagesLaparoscopic Gynecologist Surgeon in HSR Layout BangaloreDr.Beena JeysinghNo ratings yet
- Printable - Thesis On Bishop ScoreDocument103 pagesPrintable - Thesis On Bishop Scoreanuaurv100% (3)
- Gui322cpg1504e2 PDFDocument15 pagesGui322cpg1504e2 PDFieo100% (1)
- Obstetrics and Gynecology Sixth Edition Obstetrics and Gynecology Beckman Chapter 36Document8 pagesObstetrics and Gynecology Sixth Edition Obstetrics and Gynecology Beckman Chapter 363hondoNo ratings yet
- Abortion and Sterilization: Medical and Social AspectsFrom EverandAbortion and Sterilization: Medical and Social AspectsJane E. HodgsonNo ratings yet
- Surgery For Male InfertilityDocument8 pagesSurgery For Male InfertilityAkhmad MustafaNo ratings yet
- Training in Obstetrics and Gynaecology - Ippokratis SarrisDocument4 pagesTraining in Obstetrics and Gynaecology - Ippokratis Sarriszuxifoho0% (1)
- MRCOG Part 1 Exam Module SummaryDocument4 pagesMRCOG Part 1 Exam Module SummaryAmadeus KQNo ratings yet
- Sepsis in Peg Rcog PDFDocument14 pagesSepsis in Peg Rcog PDFSapna SNo ratings yet
- Poly Hi DR AmnionDocument7 pagesPoly Hi DR Amnionwanwan_adongNo ratings yet
- Ultrasound Detected Ovarian Cysts For Nuh Gynaecology TeamsDocument11 pagesUltrasound Detected Ovarian Cysts For Nuh Gynaecology TeamsDirga Rasyidin LNo ratings yet
- Tog Journal 2016Document61 pagesTog Journal 2016thevijay007100% (1)
- Operative Vaginal Delivery PDFDocument56 pagesOperative Vaginal Delivery PDFFarehan Md IsaNo ratings yet
- Endoscopy - Hysteroscopy and Laparoscopy Indications, Contraindications and ComplicationsDocument16 pagesEndoscopy - Hysteroscopy and Laparoscopy Indications, Contraindications and Complicationsselatur100% (1)
- Green Top Guidelines 13Document29 pagesGreen Top Guidelines 13garfield1No ratings yet
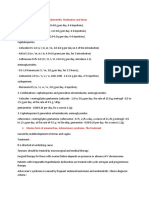
- Treatment of Acute Endometritis. Medication and DosesDocument3 pagesTreatment of Acute Endometritis. Medication and DosesTitoun LettounNo ratings yet
- Evaluation of Right Side Foetal Myocardial Performance Index in Pregestational and Gestational Diabetes MellitusDocument7 pagesEvaluation of Right Side Foetal Myocardial Performance Index in Pregestational and Gestational Diabetes MellitusGabyliz Gonzalez CastilloNo ratings yet
- Overview of Hysteroscopy - UpToDateDocument39 pagesOverview of Hysteroscopy - UpToDateCristinaCapros100% (2)
- Acog Practice Bulletin Summary: Pregestational Diabetes MellitusDocument3 pagesAcog Practice Bulletin Summary: Pregestational Diabetes MellitusMaría Fernanda Palma AcostaNo ratings yet
- FIGO Accreta Prenantal DiagnosisDocument7 pagesFIGO Accreta Prenantal DiagnosisYosef Dwi Cahyadi SalanNo ratings yet
- 2019 - Bowel and Bladder Injury Repair and Follow-Up After Gynecologic Surgery - 00006250-201902000-00012Document10 pages2019 - Bowel and Bladder Injury Repair and Follow-Up After Gynecologic Surgery - 00006250-201902000-00012Polyana FloresNo ratings yet
- E.O 51Document7 pagesE.O 51Lezirk SuercNo ratings yet
- AMTSL BrieferDocument2 pagesAMTSL BrieferNewborn2013No ratings yet
- DOPPLER ULTRASOUND IN PREGNANCYDocument64 pagesDOPPLER ULTRASOUND IN PREGNANCYHerry SasukeNo ratings yet
- Benign Disease of The UterusDocument27 pagesBenign Disease of The UterusnyangaraNo ratings yet
- ACOG Bulletin MiscarriageDocument12 pagesACOG Bulletin Miscarriagebrabba19856403No ratings yet
- Ultrasound-Guided Invasive Procedures in ObstetricsDocument18 pagesUltrasound-Guided Invasive Procedures in ObstetricsariNo ratings yet
- Management of Monochorionic Twin Pregnancy: Green-Top Guideline No. 51Document13 pagesManagement of Monochorionic Twin Pregnancy: Green-Top Guideline No. 51indra_strongNo ratings yet
- Thesis Protocol: DR - Manali Kagathara Narayanamultispeciality Hospital, JaipurDocument15 pagesThesis Protocol: DR - Manali Kagathara Narayanamultispeciality Hospital, JaipurMaitree PNo ratings yet
- Hamerlynck2018 Article FertilityOutcomeAfterTreatmentDocument7 pagesHamerlynck2018 Article FertilityOutcomeAfterTreatmentMahida El shafiNo ratings yet
- Infertility ACOGDocument8 pagesInfertility ACOGRifdaNo ratings yet
- Sign of Hyperandrogenism PDFDocument6 pagesSign of Hyperandrogenism PDFmisbah_mdNo ratings yet
- Management of Borderline Ovarian Tumors - RCOGDocument6 pagesManagement of Borderline Ovarian Tumors - RCOGYossi Agung AriosenoNo ratings yet
- Article 10.1111/tog.12576Document8 pagesArticle 10.1111/tog.12576Keeranmayeeishra0% (1)
- 1-Indroduction To EmbryologyDocument25 pages1-Indroduction To Embryologyselman P k100% (1)
- Figo ConsensusDocument44 pagesFigo ConsensusMargarita C. Ruiz HuertaNo ratings yet
- Ectopic PregnancyDocument24 pagesEctopic PregnancybertouwNo ratings yet
- Ambulatory Hysteroscopy Evidence-Based Guide To Diagnosis and TherapyDocument23 pagesAmbulatory Hysteroscopy Evidence-Based Guide To Diagnosis and TherapyAngela EstevesNo ratings yet
- Vaginal Vault ProlapseDocument9 pagesVaginal Vault ProlapseOanaNo ratings yet
- Table 4.1 AFS Classifi Cation System (: The Embryological-Clinical Classifi CationDocument111 pagesTable 4.1 AFS Classifi Cation System (: The Embryological-Clinical Classifi CationArya Syafaromania RachmaNo ratings yet
- 8surgical Management of Dysfunctional Uterine Bleeding - KabilanDocument14 pages8surgical Management of Dysfunctional Uterine Bleeding - KabilanNavani TharanNo ratings yet
- E-Poster Rcog 2018Document1 pageE-Poster Rcog 2018Ana MarianaNo ratings yet
- Effectiveness of mechanical strategies for preventing recurrent intrauterine adhesionsDocument20 pagesEffectiveness of mechanical strategies for preventing recurrent intrauterine adhesionsHarry PratamaNo ratings yet
- Vaginal Birth After Cesarean Section - Literature Review and Modern GuidelinesDocument6 pagesVaginal Birth After Cesarean Section - Literature Review and Modern GuidelinesCristinaCaprosNo ratings yet
- Ambulatory HysterosDocument8 pagesAmbulatory Hysteroskomlanihou_890233161100% (1)
- Cornual Ectopic PregnancyDocument1 pageCornual Ectopic PregnancyPavani NallaluthanNo ratings yet
- MCQ Obst Oct 2018Document22 pagesMCQ Obst Oct 2018najwan amrageaNo ratings yet
- Minimally Invasive Versus Abdominal Radical HysterectomyDocument10 pagesMinimally Invasive Versus Abdominal Radical HysterectomyClinton Franda Markus SitanggangNo ratings yet
- Preterm Labour: Management GuidelinesDocument44 pagesPreterm Labour: Management Guidelinesvacha sardarNo ratings yet
- Jurnal Inggris PDFDocument4 pagesJurnal Inggris PDFTom PrasNo ratings yet
- Hiperplasia EndometrialDocument12 pagesHiperplasia EndometrialJulián LópezNo ratings yet
- Medical Imaging TechniquesDocument96 pagesMedical Imaging TechniquesNazia WasimNo ratings yet
- Twins Discharge SummaryDocument3 pagesTwins Discharge Summarynandipati ramnadhNo ratings yet
- 17oncology1 Growth Disturbances TextsDocument28 pages17oncology1 Growth Disturbances TextsDrDeepak PawarNo ratings yet
- ACRONYMSDocument2 pagesACRONYMSDrDeepak PawarNo ratings yet
- Data Collection FormDocument2 pagesData Collection FormDrDeepak PawarNo ratings yet
- Tables and GraphsDocument17 pagesTables and GraphsDrDeepak PawarNo ratings yet
- 7-Steps For DI Systematic ApproachDocument8 pages7-Steps For DI Systematic ApproachDrDeepak Pawar71% (7)
- INTRODUCTIONDocument5 pagesINTRODUCTIONDrDeepak PawarNo ratings yet
- Methodology DMDocument3 pagesMethodology DMDrDeepak PawarNo ratings yet
- Review LiteratureDocument23 pagesReview LiteratureDrDeepak Pawar50% (4)
- Results and DiscussionDocument5 pagesResults and DiscussionDrDeepak PawarNo ratings yet
- DM Conclusion 222Document2 pagesDM Conclusion 222DrDeepak PawarNo ratings yet
- List of FiguresDocument2 pagesList of FiguresDrDeepak PawarNo ratings yet
- 10 2 33 PDFDocument4 pages10 2 33 PDFDrDeepak PawarNo ratings yet
- List of FiguresDocument2 pagesList of FiguresDrDeepak PawarNo ratings yet
- Assessing Diabetes AwarenessDocument7 pagesAssessing Diabetes AwarenessDrDeepak PawarNo ratings yet
- Chapter 3 Aim and ObjectivesDocument1 pageChapter 3 Aim and ObjectivesDrDeepak PawarNo ratings yet
- Oligo Research Article PDFDocument4 pagesOligo Research Article PDFDrDeepak PawarNo ratings yet
- Barbiturate PoisoningDocument3 pagesBarbiturate PoisoningDrDeepak PawarNo ratings yet
- Introduction to Toxicology Concepts and UnitsDocument40 pagesIntroduction to Toxicology Concepts and UnitsFauzan FasnidNo ratings yet
- Lower Respiratory Tract Infections SeminarDocument45 pagesLower Respiratory Tract Infections SeminarDrDeepak PawarNo ratings yet
- 01 M006 36157Document12 pages01 M006 36157DrDeepak PawarNo ratings yet
- Antibiotics For Upper Respiratory Tract Infections: Follow-Up Utilization and Antibiotic UseDocument5 pagesAntibiotics For Upper Respiratory Tract Infections: Follow-Up Utilization and Antibiotic UseDrDeepak PawarNo ratings yet
- A Seminar On Lower Respiratory Tract Infections: Click To Edit Master Subtitle StyleDocument44 pagesA Seminar On Lower Respiratory Tract Infections: Click To Edit Master Subtitle StyleDrDeepak PawarNo ratings yet
- Typhoid Fever AND Paratyphoid Fever: Guoli Lin Department of Infectious Diseases The Third Affiliated Hospital of SYSUDocument70 pagesTyphoid Fever AND Paratyphoid Fever: Guoli Lin Department of Infectious Diseases The Third Affiliated Hospital of SYSUDrDeepak PawarNo ratings yet
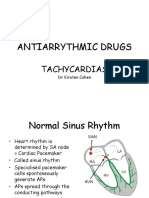
- Antiarrythmic Drugs: TachycardiasDocument36 pagesAntiarrythmic Drugs: TachycardiasDrDeepak PawarNo ratings yet
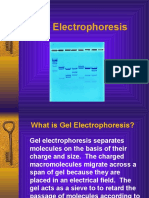
- GelelctroDocument11 pagesGelelctroDrDeepak PawarNo ratings yet
- Fish OilDocument44 pagesFish OilRamchandra Keny50% (2)
- The Potential Role of Hypocortisolism in The Pathophysiology of Stress-Related Bodily DisordersDocument35 pagesThe Potential Role of Hypocortisolism in The Pathophysiology of Stress-Related Bodily DisordersAugusto Felipe Benavides MejiasNo ratings yet
- Transcript 137 Hashimotos The Root Cause With Dr. Izabella Wentz PDFDocument26 pagesTranscript 137 Hashimotos The Root Cause With Dr. Izabella Wentz PDFPopescu AndreeaNo ratings yet
- Nccaom Biomed Exam ContentDocument12 pagesNccaom Biomed Exam Contentapi-251021152No ratings yet
- Why You Should Eat A Healthy Breakfast?Document2 pagesWhy You Should Eat A Healthy Breakfast?Lea WaskitoNo ratings yet
- Daily Lesson Log on Lifestyle and Weight ManagementDocument8 pagesDaily Lesson Log on Lifestyle and Weight ManagementNoel Isaac Maximo100% (2)
- ENIOLA CHRISTIANAH PROJECT COMPLETE RN 2022 NewDocument76 pagesENIOLA CHRISTIANAH PROJECT COMPLETE RN 2022 NewChristianahNo ratings yet
- SDS AkzoNobelDocument16 pagesSDS AkzoNobelOviedo RocíoNo ratings yet
- Fat Embolism SyndromeDocument19 pagesFat Embolism SyndromeFaizah AlmuhsinNo ratings yet
- H&S at Work act 1974 dutiesDocument44 pagesH&S at Work act 1974 dutiesSardar Majid80% (5)
- Postpartum Eclampsia Clinical Study (IJSRDocument3 pagesPostpartum Eclampsia Clinical Study (IJSRSulabh ShresthaNo ratings yet
- BP Environmental CleaningDocument250 pagesBP Environmental CleaningFaruque SathiNo ratings yet
- High Performance in Hospital Management A GuidelinDocument1 pageHigh Performance in Hospital Management A GuidelinPhương VõNo ratings yet
- Dr. Naresh NebhinaniDocument13 pagesDr. Naresh NebhinaniIlambaridhiNo ratings yet
- Nutrition Support in Adults NICE Guideline PDFDocument54 pagesNutrition Support in Adults NICE Guideline PDFnewtypeNo ratings yet
- Name: Ni Made Ayu Candra Dewi NIM: 18C10083 Class: Ilmu Keperawatan BDocument2 pagesName: Ni Made Ayu Candra Dewi NIM: 18C10083 Class: Ilmu Keperawatan BVira Permata SariNo ratings yet
- Pearson Vue 1000 File (Corrected 11-2017)Document245 pagesPearson Vue 1000 File (Corrected 11-2017)adamNo ratings yet
- Job Responsibility Checklist - RadiogrpherDocument2 pagesJob Responsibility Checklist - Radiogrphertafi66No ratings yet
- EU Vocab Extra Upper-Int 12Document2 pagesEU Vocab Extra Upper-Int 12adelinastaicaNo ratings yet
- Buletin Farmasi 11/2013Document10 pagesBuletin Farmasi 11/2013afiq83No ratings yet
- Intrenship ReviewDocument8 pagesIntrenship ReviewMLM TELUGU GAMERSNo ratings yet
- Safety Data Sheet Quorum Red Ii: Section 1. Product and Company IdentificationDocument11 pagesSafety Data Sheet Quorum Red Ii: Section 1. Product and Company IdentificationMauricio Camarena100% (1)
- Script TBDocument10 pagesScript TBMelrhean GraceNo ratings yet
- INDIVIDUAL Assignment For The Course Inclusiveness (SNIE 1012) (15%) For Engineering S and Applied A, B, & C Groups Instruction I: Choose The Best Answer For The Ten Questions That FollowDocument3 pagesINDIVIDUAL Assignment For The Course Inclusiveness (SNIE 1012) (15%) For Engineering S and Applied A, B, & C Groups Instruction I: Choose The Best Answer For The Ten Questions That FollowErmi ZuruNo ratings yet
- CÞPlMS Certification Overview and Healthcare EnvironmentDocument12 pagesCÞPlMS Certification Overview and Healthcare Environmentamarlolage100% (1)
- Frequently Asked Questions On The RH BillDocument15 pagesFrequently Asked Questions On The RH BillMulat Pinoy-Kabataan News Network100% (2)
- Interventions For Treating Post-Extraction Bleeding (Review)Document28 pagesInterventions For Treating Post-Extraction Bleeding (Review)Marcela GarciaNo ratings yet
- K4y Final EvaluationDocument9 pagesK4y Final Evaluationapi-3153554060% (1)
- Aseptic Practice Recommendations For Circulating Operating Theatre NursesDocument6 pagesAseptic Practice Recommendations For Circulating Operating Theatre NursesJudy-Anne PatricioNo ratings yet
- Menu Mspa Bali PDFDocument3 pagesMenu Mspa Bali PDFMela bali spa spaNo ratings yet