You might also like
- Endocrinology Notes for Medical StudentsFrom EverandEndocrinology Notes for Medical StudentsRating: 4 out of 5 stars4/5 (1)
- Medsurg Test 4Document11 pagesMedsurg Test 4Tori RolandNo ratings yet
- Assessment and Management of Patients With Endocrine DisordersDocument70 pagesAssessment and Management of Patients With Endocrine Disordersۦۦ JamesNo ratings yet
- Hyperthyroidism 2011Document30 pagesHyperthyroidism 2011Elyza MagsaysayNo ratings yet
- Assessment and Management of Patients With Endocrine DisordersDocument78 pagesAssessment and Management of Patients With Endocrine Disordershenny1620100% (1)
- HipotiroidDocument27 pagesHipotiroidJuwitaNo ratings yet
- Pituitary DisorderDocument34 pagesPituitary DisorderSoniya ShivanshNo ratings yet
- The Endocrine Systyem NDocument93 pagesThe Endocrine Systyem NMuh YaminNo ratings yet
- Endocrine Dysfunction: Adrenal & Pituitary: Endocrine System Endocrine ReviewDocument102 pagesEndocrine Dysfunction: Adrenal & Pituitary: Endocrine System Endocrine ReviewCalimlim KimNo ratings yet
- Diseases of The Endocrine SystemDocument7 pagesDiseases of The Endocrine SystemJaeLene DacwagNo ratings yet
- U World Endocrine FinalDocument12 pagesU World Endocrine Finalsean blazeNo ratings yet
- 40.43.function of Endocrine - Pptx?targetDocument28 pages40.43.function of Endocrine - Pptx?targetAnnemerline RavixNo ratings yet
- Thyroid Disorders: Hyperthyroidism HypothyroidismDocument66 pagesThyroid Disorders: Hyperthyroidism HypothyroidismGabz GabbyNo ratings yet
- Endocrine Disorders TableDocument6 pagesEndocrine Disorders TablebarbaraNo ratings yet
- SC2 2015 HyperthyroidismDocument38 pagesSC2 2015 HyperthyroidismShafern TanNo ratings yet
- Hypo ThyroidismDocument7 pagesHypo ThyroidismAnne Alejo-Leal100% (1)
- Thyroid ParathyroidDocument79 pagesThyroid Parathyroid2M SANCHEZ, CYLESNo ratings yet
- Hyperthyroid Is Med ItDocument31 pagesHyperthyroid Is Med ItJuliana Sanjaya VocNo ratings yet
- Askep GGN ThyroidDocument26 pagesAskep GGN ThyroidTsaalits MuharrorohNo ratings yet
- Assessment of Endocrine System: History TakingDocument14 pagesAssessment of Endocrine System: History TakingNida Naaz100% (2)
- RNSG 1533 Raising The Bar For Success Concept: Metabolism: Diabetes Type 1/diabetes Type 2Document4 pagesRNSG 1533 Raising The Bar For Success Concept: Metabolism: Diabetes Type 1/diabetes Type 2katrinasdNo ratings yet
- Endocrine Disorders PDFDocument6 pagesEndocrine Disorders PDFShelleyNo ratings yet
- Thyroid Disease Is Relatively Common, With A Gender Predisposition To FemalesDocument3 pagesThyroid Disease Is Relatively Common, With A Gender Predisposition To FemalesCharmaine SolimanNo ratings yet
- DwarfismDocument5 pagesDwarfismjasminemuammilNo ratings yet
- Endocrine System 2Document7 pagesEndocrine System 2Lhaura Joy ArsenioNo ratings yet
- Disorders of The Thyroid1Document22 pagesDisorders of The Thyroid1Saddamix AL OmariNo ratings yet
- Hypothyroidism: Neysa Ornella D 17-102Document18 pagesHypothyroidism: Neysa Ornella D 17-102Neysa Ornella DiraNo ratings yet
- Thyroid Gland Diseases in Children-1Document36 pagesThyroid Gland Diseases in Children-1Jeffrey EkaNo ratings yet
- 1 - Endocrine DisordersDocument55 pages1 - Endocrine Disorderscephas chinkoliNo ratings yet
- Endocrine DisodersDocument330 pagesEndocrine Disodersbrianmuthomi851No ratings yet
- Pathophysiology of Endocrine SystemDocument64 pagesPathophysiology of Endocrine SystemTess MohamedNo ratings yet
- Thyroid LectureDocument65 pagesThyroid LectureAndres TabaresNo ratings yet
- Causes of Hyperthyroidism2Document73 pagesCauses of Hyperthyroidism2Kompari EvansNo ratings yet
- Thyroid Gland: Dr. Humairah Medina Liza Lubis, M. Ked (PA), SP - PADocument138 pagesThyroid Gland: Dr. Humairah Medina Liza Lubis, M. Ked (PA), SP - PARizky anandaNo ratings yet
- Thyroid DisordersDocument66 pagesThyroid DisordersJOY SANDHYA JOSEPH (RA2123003011002)No ratings yet
- SC2 2015 HypothyroidismDocument23 pagesSC2 2015 HypothyroidismShafern TanNo ratings yet
- Thyroid Disorders in ChildrenDocument30 pagesThyroid Disorders in ChildrenZm100% (1)
- HyperthyroidDocument5 pagesHyperthyroidJameston BostreNo ratings yet
- ArainDocument71 pagesArainAllah Bux KhosoNo ratings yet
- Hyperthyroidism: Sudiarto, MNDocument21 pagesHyperthyroidism: Sudiarto, MNerikaNo ratings yet
- Thyroid DisordersDocument61 pagesThyroid DisordersdrmamodoNo ratings yet
- Pituitary GlandDocument9 pagesPituitary GlandS GrayNo ratings yet
- Kelainan TyroidDocument20 pagesKelainan TyroidAnnisa Aulia RakhmahNo ratings yet
- Thyroid DisordersDocument55 pagesThyroid DisordersNsubuga Ivan100% (1)
- Aging and Endocrine DisordersDocument23 pagesAging and Endocrine DisordersadystiNo ratings yet
- Assessment and Management of Patients With Endocrine DisordersDocument55 pagesAssessment and Management of Patients With Endocrine Disorderseliza marie luisNo ratings yet
- 7.3 Endocrine Disorders PPTDocument36 pages7.3 Endocrine Disorders PPTLorelie AsisNo ratings yet
- Hyperthyroidism in Cats: Typical Clinical SignsDocument5 pagesHyperthyroidism in Cats: Typical Clinical Signscarteparte100% (1)
- 6.1 Pitutary DisorderDocument32 pages6.1 Pitutary Disordersiltanu awokeNo ratings yet
- EndocrinologyDocument50 pagesEndocrinologyCut TirayaNo ratings yet
- Endocrine Disorders: Aprilia Indra K, M.BiotechDocument36 pagesEndocrine Disorders: Aprilia Indra K, M.BiotechFifiana AngeliaNo ratings yet
- ST 25Document125 pagesST 25hassanNo ratings yet
- Thyroid Disorders1Document67 pagesThyroid Disorders1AzeemNo ratings yet
- Chapter 45 Endocrine DosordersDocument50 pagesChapter 45 Endocrine DosordersShaun Gabriel AmpoNo ratings yet
- Lewis: Medical-Surgical Nursing, 8th Edition: Chapter 50: Nursing Management: Endocrine Problems Key Points - PrintableDocument7 pagesLewis: Medical-Surgical Nursing, 8th Edition: Chapter 50: Nursing Management: Endocrine Problems Key Points - Printablelpirman05No ratings yet
- HyperthyroidismDocument54 pagesHyperthyroidismAsiah JelitaNo ratings yet
- Endocrinology-II Past Papers 3rd Year-1Document11 pagesEndocrinology-II Past Papers 3rd Year-1Syed Muhammad HameemNo ratings yet
- Thyroid Disease: Hyperthyroidism: The most important information you need to improve your healthFrom EverandThyroid Disease: Hyperthyroidism: The most important information you need to improve your healthRating: 1 out of 5 stars1/5 (1)
- Hyperthyroidism, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandHyperthyroidism, A Simple Guide To The Condition, Treatment And Related ConditionsRating: 2 out of 5 stars2/5 (2)
- EliteSchedule16 17mar172017 PDFDocument1 pageEliteSchedule16 17mar172017 PDFRosemaryCastroNo ratings yet
- Hormonal Physiology of Childbearing PDFDocument248 pagesHormonal Physiology of Childbearing PDFRosemaryCastro100% (1)
- FREESchool Supply LabelsDocument1 pageFREESchool Supply LabelsRosemaryCastroNo ratings yet
- OB ReviewDocument257 pagesOB ReviewRosemaryCastro100% (1)
- Hormonal Physiology of Childbearing PDFDocument248 pagesHormonal Physiology of Childbearing PDFRosemaryCastro100% (1)
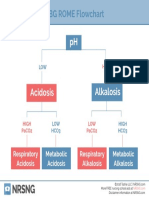
- ABG ROME FlowchartDocument1 pageABG ROME FlowchartRosemaryCastro100% (1)
- IV Solutions CheatsheetDocument1 pageIV Solutions CheatsheetRosemaryCastroNo ratings yet
- PHN SAMPLE AppDocument3 pagesPHN SAMPLE AppRosemaryCastroNo ratings yet
- NRP GeneralDocument1 pageNRP GeneralRosemaryCastroNo ratings yet
- SIM Lab Sign UpsDocument3 pagesSIM Lab Sign UpsRosemaryCastroNo ratings yet
- And The School Bell Rings For Spring 16: Welcome To Second Semester!Document4 pagesAnd The School Bell Rings For Spring 16: Welcome To Second Semester!RosemaryCastroNo ratings yet
- Monthly Shot January 2016Document7 pagesMonthly Shot January 2016RosemaryCastroNo ratings yet
- Where Have I Been While in NURSING SCHOOL?: Résumé Worksheet Belonging To - Save MeDocument2 pagesWhere Have I Been While in NURSING SCHOOL?: Résumé Worksheet Belonging To - Save MeRosemaryCastroNo ratings yet
- National Travel Fund Application1Document2 pagesNational Travel Fund Application1RosemaryCastroNo ratings yet
- Club Agreement FormDocument4 pagesClub Agreement FormRosemaryCastroNo ratings yet
- Chlamydia: California Department of Public HealthDocument12 pagesChlamydia: California Department of Public HealthRosemaryCastroNo ratings yet
- N144 Peer Evaluation Rosemary CastroDocument2 pagesN144 Peer Evaluation Rosemary CastroRosemaryCastroNo ratings yet
- Team #: 2 Names of Health Education Project Group Members Who Worked On This In-Class Activity: Rosemary Castro, Lachelle Manalo ObjectivesDocument2 pagesTeam #: 2 Names of Health Education Project Group Members Who Worked On This In-Class Activity: Rosemary Castro, Lachelle Manalo ObjectivesRosemaryCastroNo ratings yet
- Nursing School Weeks 9-16Document2 pagesNursing School Weeks 9-16RosemaryCastroNo ratings yet
- A Review and Current Situation of Pcos With InfertilityDocument15 pagesA Review and Current Situation of Pcos With InfertilityIJAR JOURNALNo ratings yet
- Physioex Lab Report: Pre-Lab Quiz ResultsDocument13 pagesPhysioex Lab Report: Pre-Lab Quiz ResultsIvana FNo ratings yet
- Phlebo India 659Document2 pagesPhlebo India 659Dharma GagganapallyNo ratings yet
- Diet TiroidDocument6 pagesDiet TiroidAhmad Umar AfNo ratings yet
- Hypothyroidism - Practice Essentials, Background, PathophysiologyDocument17 pagesHypothyroidism - Practice Essentials, Background, PathophysiologyprobowurNo ratings yet
- Thyroiditis: What Is The Thyroid Gland?Document3 pagesThyroiditis: What Is The Thyroid Gland?Angga M RahmanNo ratings yet
- Big Group A1 General Task 1 Nursing AssessmentDocument15 pagesBig Group A1 General Task 1 Nursing AssessmentCAUSIN, Lance Matthew,No ratings yet
- Hair Analysis Interpretation Guide: The Eck Institute. Issue 27-29Document2 pagesHair Analysis Interpretation Guide: The Eck Institute. Issue 27-29Jianhua Shi100% (1)
- Approach To The Patient With Delayed Puberty - UpToDateDocument47 pagesApproach To The Patient With Delayed Puberty - UpToDateCristinaCaprosNo ratings yet
- Thyroid Function TestsDocument21 pagesThyroid Function TestsPraneeth TirumalasettyNo ratings yet
- Disorders of The Thyroid and Parathyroid Glands: Ms TeamDocument36 pagesDisorders of The Thyroid and Parathyroid Glands: Ms TeamShy Dela PuertaNo ratings yet
- Endocrine System WorksheetDocument2 pagesEndocrine System WorksheetshasagailNo ratings yet
- Rietz Thyroid Final PDFDocument50 pagesRietz Thyroid Final PDFRoberto CortezNo ratings yet
- Laboratory ValuesDocument12 pagesLaboratory ValuesJaney Co100% (2)
- Hashimoto and Grave DiseaseDocument9 pagesHashimoto and Grave DiseaseNadia ElaizaNo ratings yet
- Hormones and Related DrugsDocument42 pagesHormones and Related DrugsRamya PrabhuNo ratings yet
- Sashikant Modi Comprehensive Full Body Checkup Includes 107 Tests 12092017 131456Document9 pagesSashikant Modi Comprehensive Full Body Checkup Includes 107 Tests 12092017 131456Sashikant ModiNo ratings yet
- CholeDocument12 pagesCholeaquacrystal538No ratings yet
- Metabolic and Endocrine ManagementDocument42 pagesMetabolic and Endocrine ManagementAlyssa MontimorNo ratings yet
- PathophysiologyDocument7 pagesPathophysiologyAko Si Vern ÖNo ratings yet
- Hashimoto's Thyroiditis: Veena RedkarDocument10 pagesHashimoto's Thyroiditis: Veena RedkarSan RedkarNo ratings yet
- Family Medicine FinalDocument35 pagesFamily Medicine Finalzdfdgsdgsh sggaesgs0% (1)
- Hypothyroidism - Harrison Copy-PasteDocument4 pagesHypothyroidism - Harrison Copy-PasteJoseph De Joya100% (1)
- Kuliah Tiroid (Prof - Dr. Harsinen S, SP - pd-kEMD)Document138 pagesKuliah Tiroid (Prof - Dr. Harsinen S, SP - pd-kEMD)aliimranzNo ratings yet
- Endocrine SystemDocument6 pagesEndocrine SystemChechan AmbaNo ratings yet
- BHTbook StevenWmFowkes 141016Document67 pagesBHTbook StevenWmFowkes 141016Sparklight JackNo ratings yet
- Autoimmune Diseases in PregnancyDocument42 pagesAutoimmune Diseases in PregnancyDr_Soranus100% (1)
- 2 - Thyroxine and Treatment of Hypothyroidism - 2019Document8 pages2 - Thyroxine and Treatment of Hypothyroidism - 2019Johanna Bustos NutricionistaNo ratings yet
- Haematology Basic Screening Package Complete Blood Count (CBC EXT)Document6 pagesHaematology Basic Screening Package Complete Blood Count (CBC EXT)Anil PeshinNo ratings yet
- Thyroid DisordersDocument67 pagesThyroid DisordersMA 09No ratings yet