You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Tetralogy of Fallot ExplainedDocument31 pagesTetralogy of Fallot ExplainedDevipriya MajumderNo ratings yet
- Monster Lore - Priest of BlightDocument2 pagesMonster Lore - Priest of BlightNorak31No ratings yet
- EditorialDocument7 pagesEditorialapi-450098246No ratings yet
- RBI Sees 9.5 PC GDP Contraction in FY21: India S Active Covid-19 Cases Fall Below 9 LakhDocument12 pagesRBI Sees 9.5 PC GDP Contraction in FY21: India S Active Covid-19 Cases Fall Below 9 LakhGauravNo ratings yet
- General Veterinary Parasitology and Helminthology PDFDocument253 pagesGeneral Veterinary Parasitology and Helminthology PDFLakshmi75% (4)
- XL MulticalDocument2 pagesXL MulticalĐào Huy VănNo ratings yet
- Hygienic Milk Collection and Testing PDFDocument32 pagesHygienic Milk Collection and Testing PDFAhmad Fariz Maulana100% (1)
- Plab September 2015 Recalls by Samia NazDocument7 pagesPlab September 2015 Recalls by Samia NazDr-Jahanzaib GondalNo ratings yet
- Penyuluhan-Faktor Risiko Dislipidemia - FixDocument39 pagesPenyuluhan-Faktor Risiko Dislipidemia - FixAisyahNurjannah100% (1)
- Protozoa Classification and CharacteristicsDocument3 pagesProtozoa Classification and CharacteristicsTrisha AlejandroNo ratings yet
- Full Speech by President Gotabaya Rajapaksa at "The Future of Asia" ConferenceDocument10 pagesFull Speech by President Gotabaya Rajapaksa at "The Future of Asia" ConferenceAdaderana OnlineNo ratings yet
- Draft Research ProposalDocument5 pagesDraft Research ProposalNursakmawani Abdul RafarNo ratings yet
- Filariasis: Signs and SymptomsDocument30 pagesFilariasis: Signs and SymptomsAnonymous VJjzqbAlNo ratings yet
- PREDICT Lab Protocols UC 1, 2 Mar 2013 PDFDocument286 pagesPREDICT Lab Protocols UC 1, 2 Mar 2013 PDFEver CordovaNo ratings yet
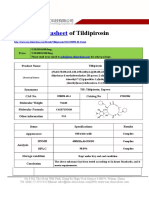
- Datasheet of Tildipirosin - CAS 328898-40-4Document2 pagesDatasheet of Tildipirosin - CAS 328898-40-4LouisNo ratings yet
- Environmental Cleaning APSIC Guideline 14 Jan 2013Document128 pagesEnvironmental Cleaning APSIC Guideline 14 Jan 2013Suprapto W100% (1)
- Spanish Flu HistoryDocument3 pagesSpanish Flu Historyrichlion50% (6)
- Statistics and Propaganda: by Jon RappoportDocument6 pagesStatistics and Propaganda: by Jon RappoportSkogspilen Sprett100% (1)
- DPH Governor General Programme 2017 FinalDocument6 pagesDPH Governor General Programme 2017 Finalterry johnsonNo ratings yet
- Girlscout of The Philippines: Basista National High School Basista, PangasinanDocument3 pagesGirlscout of The Philippines: Basista National High School Basista, PangasinanLj Cortez CagunotNo ratings yet
- Crude, Specific & Adjusted Rates DefinedDocument19 pagesCrude, Specific & Adjusted Rates Definedjaish8904100% (1)
- DiphenhydramineDocument6 pagesDiphenhydramineAndrea BroccoliNo ratings yet
- Lorenzo v. Director of HealthDocument1 pageLorenzo v. Director of HealthYeyen M. EvoraNo ratings yet
- The Changing Face of India 1Document2 pagesThe Changing Face of India 1Kartik BansalNo ratings yet
- VLBW Newborn Resuscitation: Pros and Cons: Yousef K. Abu-Osba, M.DDocument26 pagesVLBW Newborn Resuscitation: Pros and Cons: Yousef K. Abu-Osba, M.DVicky HadiNo ratings yet
- Block 4 Lung PathDocument31 pagesBlock 4 Lung PathShalini ShanmugalingamNo ratings yet
- Case Report SleDocument37 pagesCase Report SleUswah SudirmanNo ratings yet
- Retinal Diseases - 5Document2 pagesRetinal Diseases - 5AkicaNo ratings yet
- North of England P&I Signals-106 2017 - 03 PDFDocument12 pagesNorth of England P&I Signals-106 2017 - 03 PDFToheid AsadiNo ratings yet